

Counteracting learned non-use in chronic stroke patients with reinforcement-induced movement therapy
- PMID: 27506203
- PMCID: PMC4979116
- DOI: 10.1186/s12984-016-0178-x
Counteracting learned non-use in chronic stroke patients with reinforcement-induced movement therapy
Abstract
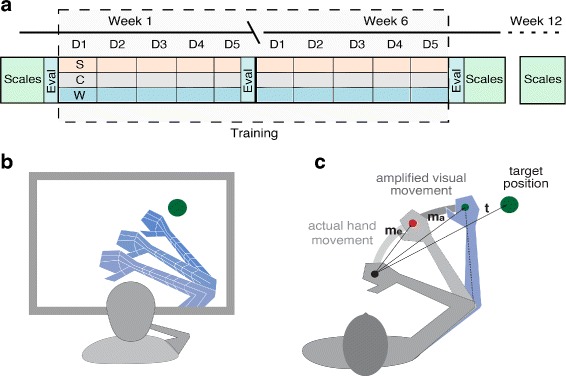
Background: After stroke, patients who suffer from hemiparesis tend to suppress the use of the affected extremity, a condition called learned non-use. Consequently, the lack of training may lead to the progressive deterioration of motor function. Although Constraint-Induced Movement Therapies (CIMT) have shown to be effective in treating this condition, the method presents several limitations, and the high intensity of its protocols severely compromises its adherence. We propose a novel rehabilitation approach called Reinforcement-Induced Movement Therapy (RIMT), which proposes to restore motor function through maximizing arm use. This is achieved by exposing the patient to amplified goal-oriented movements in VR that match the intended actions of the patient. We hypothesize that through this method we can increase the patients self-efficacy, reverse learned non-use, and induce long-term motor improvements.
Methods: We conducted a randomized, double-blind, longitudinal clinical study with 18 chronic stroke patients. Patients performed 30 minutes of daily VR-based training during six weeks. During training, the experimental group experienced goal-oriented movement amplification in VR. The control group followed the same training protocol but without movement amplification. Evaluators blinded to group designation performed clinical measurements at the beginning, at the end of the training and at 12-weeks follow-up. We used the Fugl-Meyer Assessment for the upper extremities (UE-FM) (Sanford et al., Phys Ther 73:447-454, 1993) as a primary outcome measurement of motor recovery. Secondary outcome measurements included the Chedoke Arm and Hand Activity Inventory (CAHAI-7) (Barreca et al., Arch Phys Med Rehabil 6:1616-1622, 2005) for measuring functional motor gains in the performance of Activities of Daily Living (ADLs), the Barthel Index (BI) for the evaluation of the patient's perceived independence (Collin et al., Int Disabil Stud 10:61-63, 1988), and the Hamilton scale (Knesevich et al., Br J Psychiatr J Mental Sci 131:49-52, 1977) for the identification of improvements in mood disorders that could be induced by the reinforcement-based intervention. In order to study and predict the effects of this intervention we implemented a computational model of recovery after stroke.
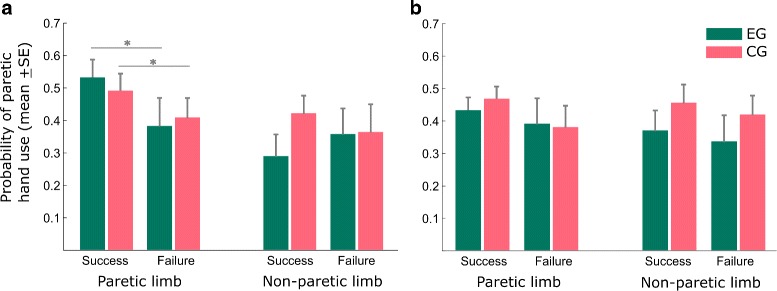
Results: While both groups showed significant motor gains at 6-weeks post-treatment, only the experimental group continued to exhibit further gains in UE-FM at 12-weeks follow-up (p<.05). This improvement was accompanied by a significant increase in arm-use during training in the experimental group.
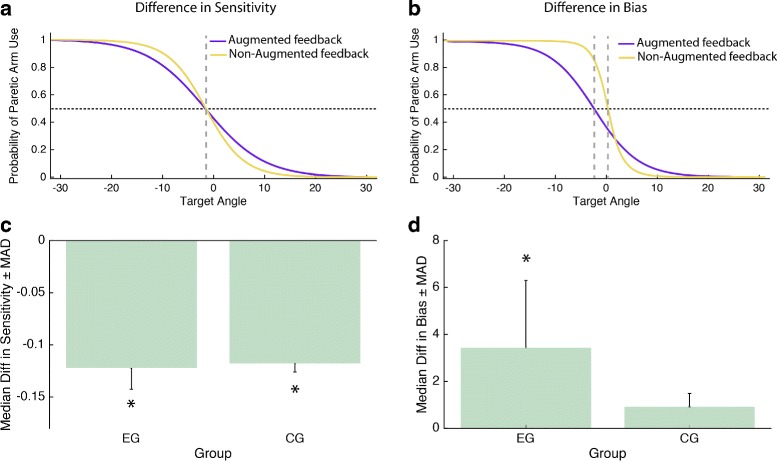
Conclusions: Implicitly reinforcing arm-use by augmenting visuomotor feedback as proposed by RIMT seems beneficial for inducing significant improvement in chronic stroke patients. By challenging the patients' self-limiting believe system and perceived low self-efficacy this approach might counteract learned non-use.
Trial registration: Clinical Trials NCT02657070 .
Keywords: Deductive medicine; Learned non-use; Rehabilitation; Stroke; Virtual reality.
Figures



References
-
- Taub E, Uswatte G, Mark VW, Morris DMM. The learned nonuse phenomenon: implications for rehabilitation. Europa Medicophysica. 2006;42(3):241–56. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
