

Use of Electronic Health Data to Estimate Heart Failure Events in a Population-Based Cohort with CKD
- PMID: 27507770
- PMCID: PMC5108195
- DOI: 10.2215/CJN.03900416
Use of Electronic Health Data to Estimate Heart Failure Events in a Population-Based Cohort with CKD
Abstract
Background and objectives: Studies that use electronic health data typically identify heart failure (HF) events from hospitalizations with a principal diagnosis of HF. This approach may underestimate the total burden of HF among persons with CKD. We assessed the accuracy of algorithms for identifying validated HF events from hospitalizations and outpatient encounters, and we used this validation information to estimate the rate of HF events in a large CKD population.
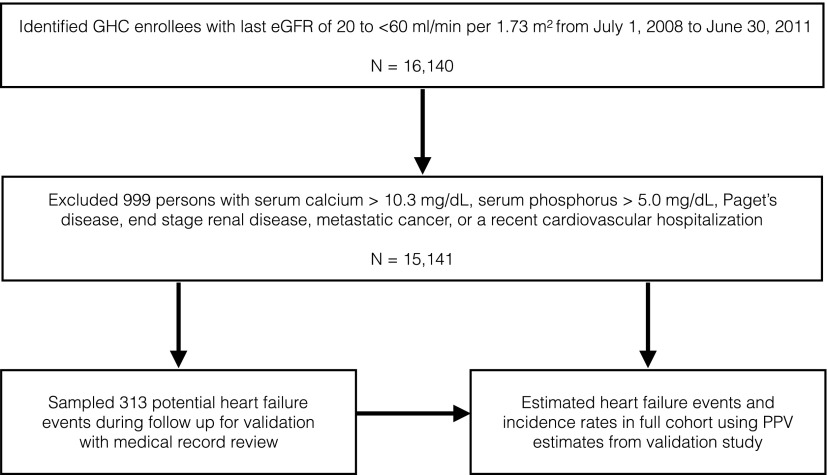
Design, setting, participants, & measurements: We identified a cohort of 15,141 adults age 18-89 years with an eGFR<60 ml/min per 1.73 m2 from 2008 to 2011. Potential HF events during follow-up were randomly sampled for validation with medical record review. Positive predictive values from the validation study were used to estimate the rate of validated HF events in the full cohort.
Results: A total of 1864 participants had at least one health care encounter that qualified as a potential HF event during 2.7 years of mean follow-up. Among 313 potential events that were randomly sampled for validation, positive predictive values were 92% for hospitalizations with a principal diagnosis of HF, 32% for hospitalizations with a secondary diagnosis of HF, and 70% for qualifying outpatient HF encounters. Through use of this validation information in the full cohort, the rate of validated HF events estimated from the most comprehensive algorithm that included principal and secondary diagnosis hospitalizations and outpatient encounters was 35.2 events/1000 person-years (95% confidence interval, 33.1 to 37.4), compared with 9.5 events/1000 person-years (95% confidence interval, 8.7 to 10.5) from the algorithm that included only principal diagnosis hospitalizations. Outpatient encounters accounted for 20% of the total number of validated HF events.
Conclusions: In studies that rely on electronic health data, algorithms that include hospitalizations with a secondary diagnosis of HF and outpatient HF encounters more fully capture the burden of HF, although validation of HF events may be necessary with this approach.
Keywords: EGFR protein, human; adult; algorithms; chronic kidney disease; electronic health records; epidemiology and outcomes; follow-up studies; heart failure; hospitalization; humans; medical records; outpatients; receptor, epidermal growth factor.
Copyright © 2016 by the American Society of Nephrology.
Figures
References
-
- Levey AS, Coresh J: Chronic kidney disease. Lancet 379: 165–180, 2012 - PubMed
-
- Gansevoort RT, Correa-Rotter R, Hemmelgarn BR, Jafar TH, Heerspink HJ, Mann JF, Matsushita K, Wen CP: Chronic kidney disease and cardiovascular risk: Epidemiology, mechanisms, and prevention. Lancet 382: 339–352, 2013 - PubMed
-
- Go AS, Chertow GM, Fan D, McCulloch CE, Hsu CY: Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N Engl J Med 351: 1296–1305, 2004 - PubMed
-
- Matsushita K, van der Velde M, Astor BC, Woodward M, Levey AS, de Jong PE, Coresh J, Gansevoort RT; Chronic Kidney Disease Prognosis Consortium : Association of estimated glomerular filtration rate and albuminuria with all-cause and cardiovascular mortality in general population cohorts: A collaborative meta-analysis. Lancet 375: 2073–2081, 2010 - PMC - PubMed
-
- Sarnak MJ, Katz R, Stehman-Breen CO, Fried LF, Jenny NS, Psaty BM, Newman AB, Siscovick D, Shlipak MG; Cardiovascular Health Study : Cystatin C concentration as a risk factor for heart failure in older adults. Ann Intern Med 142: 497–505, 2005 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
