

Differential Response to Low-Dose Dopamine or Low-Dose Nesiritide in Acute Heart Failure With Reduced or Preserved Ejection Fraction: Results From the ROSE AHF Trial (Renal Optimization Strategies Evaluation in Acute Heart Failure)
- PMID: 27512103
- PMCID: PMC5034712
- DOI: 10.1161/CIRCHEARTFAILURE.115.002593
Differential Response to Low-Dose Dopamine or Low-Dose Nesiritide in Acute Heart Failure With Reduced or Preserved Ejection Fraction: Results From the ROSE AHF Trial (Renal Optimization Strategies Evaluation in Acute Heart Failure)
Abstract
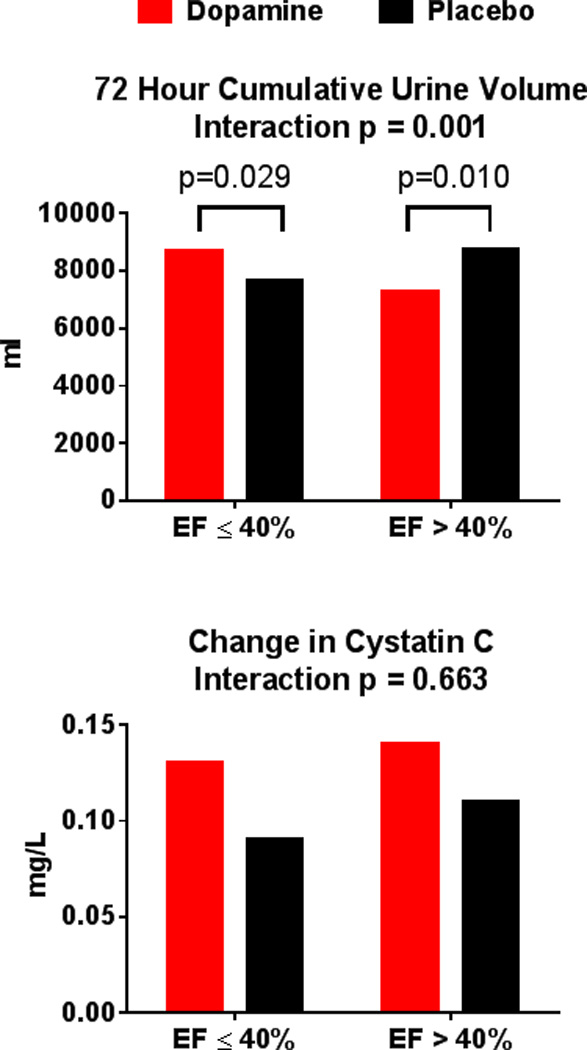
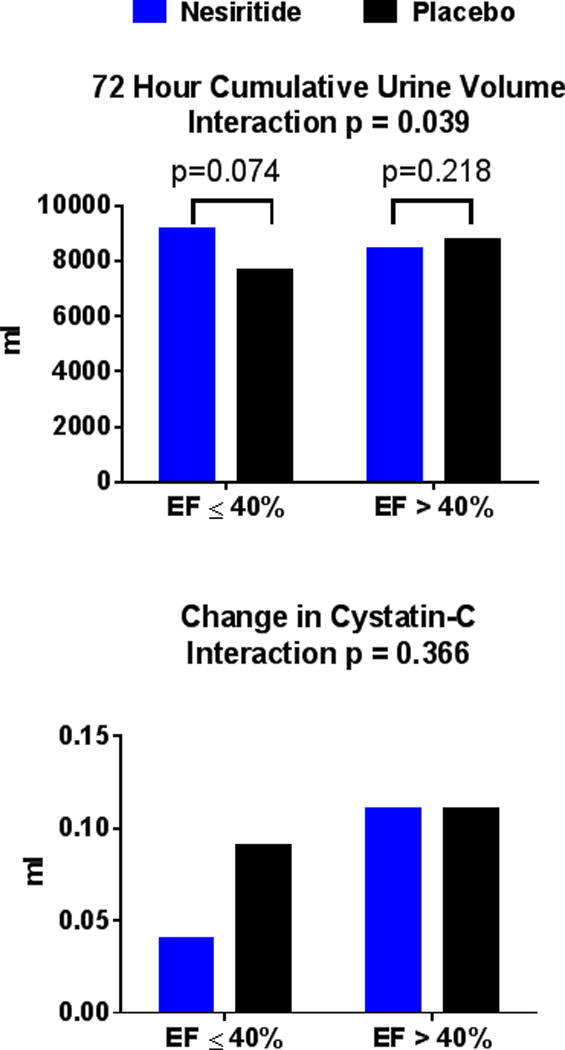
Background: The ROSE AHF trial (Renal Optimization Strategies Evaluation in Acute Heart Failure) found that when compared with placebo, neither low-dose dopamine (2 µg/kg per minute) nor low-dose nesiritide (0.005 μg/kg per minute without bolus) enhanced decongestion or preserved renal function in AHF patients with renal dysfunction. However, there may be differential responses to vasoactive agents in AHF patients with reduced versus preserved ejection fraction (EF). This post hoc analysis examined potential interaction between treatment effect and EF (EF ≤40% versus >40%) on the ROSE AHF end points.
Methods and results: ROSE AHF enrolled AHF patients (n=360; any EF) with renal dysfunction. The coprimary end points were cumulative urine volume and the change in serum cystatin-C in 72 hours. The effect of dopamine (interaction P=0.001) and nesiritide (interaction P=0.039) on urine volume varied by EF group. In heart failure with reduced EF, urine volume was higher with active treatment versus placebo, whereas in heart failure with preserved EF, urine volume was lower with active treatment. The effect of dopamine and nesiritide on weight change, sodium excretion, and incidence of AHF treatment failure also varied by EF group (interaction P<0.05 for all). There was no interaction between vasoactive treatment's effect and EF on change in cystatin-C. Compared with placebo, dopamine was associated with improved clinical outcomes in heart failure with reduced EF and worse clinical outcomes in heart failure with preserved EF. With nesiritide, there were no differences in clinical outcomes when compared with placebo in both heart failure with reduced EF and heart failure with preserved EF.
Conclusions: In this post hoc analysis of ROSE AHF, the response to vasoactive therapies differed in patients with heart failure with reduced EF and heart failure with preserved EF. Investigations of AHF therapies should assess the potential for differential responses in AHF with preserved versus reduced EF.
Clinical trial registration: URL: http://www.clinicaltrials.gov. Unique identifier: NCT01132846.
Keywords: dopamine; heart failure; humans; incidence; kidney; natriuretic peptide, brain.
© 2016 American Heart Association, Inc.
Figures
Similar articles
-
Low-dose dopamine or low-dose nesiritide in acute heart failure with renal dysfunction: the ROSE acute heart failure randomized trial.JAMA. 2013 Dec 18;310(23):2533-43. doi: 10.1001/jama.2013.282190. JAMA. 2013. PMID: 24247300 Free PMC article. Clinical Trial.
-
Is there still a role for low-dose dopamine use in acute heart failure?Curr Opin Crit Care. 2014 Oct;20(5):467-71. doi: 10.1097/MCC.0000000000000133. Curr Opin Crit Care. 2014. PMID: 25137402 Review.
-
Effects of standard heart failure therapy and concomitant treatment with intravenous furosemide or inotropes (dobutamine, dopamine, and/or milrinone) on renal function and mortality in patients treated with nesiritide.Am J Cardiol. 2006 Dec 15;98(12):1627-30. doi: 10.1016/j.amjcard.2006.07.044. Epub 2006 Oct 25. Am J Cardiol. 2006. PMID: 17145223
-
Low-dose nesiritide improves renal function in heart failure patients following acute myocardial infarction.Heart Vessels. 2010 Mar;25(2):97-103. doi: 10.1007/s00380-009-1171-0. Epub 2010 Mar 26. Heart Vessels. 2010. PMID: 20339970 Clinical Trial.
-
ROSE-AHF and lessons learned.Curr Heart Fail Rep. 2014 Sep;11(3):260-5. doi: 10.1007/s11897-014-0208-6. Curr Heart Fail Rep. 2014. PMID: 24966060 Free PMC article. Review.
Cited by
-
Pathophysiology and Therapeutic Approaches to Acute Decompensated Heart Failure.Circ Res. 2021 May 14;128(10):1468-1486. doi: 10.1161/CIRCRESAHA.121.318186. Epub 2021 May 13. Circ Res. 2021. PMID: 33983837 Free PMC article. Review.
-
Congestion in Heart Failure: From the Secret of a Mummy to Today's Novel Diagnostic and Therapeutic Approaches: A Comprehensive Review.J Clin Med. 2023 Dec 19;13(1):12. doi: 10.3390/jcm13010012. J Clin Med. 2023. PMID: 38202020 Free PMC article. Review.
-
Neurohormonal Effects of Intravenous Dopamine in Patients with Acute Heart Failure.J Clin Med. 2024 Sep 24;13(19):5667. doi: 10.3390/jcm13195667. J Clin Med. 2024. PMID: 39407727 Free PMC article.
-
Lower urine sodium predicts longer length of stay in acute heart failure patients: Insights from the ROSE AHF trial.Clin Cardiol. 2020 Jan;43(1):43-49. doi: 10.1002/clc.23286. Epub 2019 Nov 12. Clin Cardiol. 2020. PMID: 31721249 Free PMC article. Clinical Trial.
-
Efficacy of Nondiuretic Pharmacotherapy for Improving the Treatment of Congestion in Patients with Acute Heart Failure: A Systematic Review of Randomised Controlled Trials.J Clin Med. 2022 May 31;11(11):3112. doi: 10.3390/jcm11113112. J Clin Med. 2022. PMID: 35683505 Free PMC article. Review.
References
-
- Mozaffarian D, Benjamin EJ, Go AS, Arnett DK, Blaha MJ, Cushman M, de Ferranti S, Despres JP, Fullerton HJ, Howard VJ, Huffman MD, Judd SE, Kissela BM, Lackland DT, Lichtman JH, Lisabeth LD, Liu S, Mackey RH, Matchar DB, McGuire DK, Mohler ER, 3rd, Moy CS, Muntner P, Mussolino ME, Nasir K, Neumar RW, Nichol G, Palaniappan L, Pandey DK, Reeves MJ, Rodriguez CJ, Sorlie PD, Stein J, Towfighi A, Turan TN, Virani SS, Willey JZ, Woo D, Yeh RW, Turner MB. Heart disease and stroke statistics-2015 update: A report from the american heart association. Circulation. 2015;131:e29–e322. - PubMed
-
- Gheorghiade M, Zannad F, Sopko G, Klein L, Pina IL, Konstam MA, Massie BM, Roland E, Targum S, Collins SP, Filippatos G, Tavazzi L. Acute heart failure syndromes: Current state and framework for future research. Circulation. 2005;112:3958–3968. - PubMed
-
- Yancy CW, Lopatin M, Stevenson LW, De Marco T, Fonarow GC. Clinical presentation, management, and in-hospital outcomes of patients admitted with acute decompensated heart failure with preserved systolic function: A report from the acute decompensated heart failure national registry (adhere) database. J Am Coll Cardiol. 2006;47:76–84. - PubMed
-
- Chen HH, Anstrom KJ, Givertz MM, Stevenson LW, Semigran MJ, Goldsmith SR, Bart BA, Bull DA, Stehlik J, LeWinter MM, Konstam MA, Huggins GS, Rouleau JL, O'Meara E, Tang WH, Starling RC, Butler J, Deswal A, Felker GM, O'Connor CM, Bonita RE, Margulies KB, Cappola TP, Ofili EO, Mann DL, Davila-Roman VG, McNulty SE, Borlaug BA, Velazquez EJ, Lee KL, Shah MR, Hernandez AF, Braunwald E, Redfield MM. Low-dose dopamine or low-dose nesiritide in acute heart failure with renal dysfunction: The rose acute heart failure randomized trial. Jama. 2013;310:2533–2543. - PMC - PubMed
-
- Cotter G, Weissgarten J, Metzkor E, Moshkovitz Y, Litinski I, Tavori U, Perry C, Zaidenstein R, Golik A. Increased toxicity of high-dose furosemide versus low-dose dopamine in the treatment of refractory congestive heart failure. Clin Pharmacol Ther. 1997;62:187–193. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- U01 HL084890/HL/NHLBI NIH HHS/United States
- U01 HL084891/HL/NHLBI NIH HHS/United States
- U54 MD007588/MD/NIMHD NIH HHS/United States
- U01 HL084931/HL/NHLBI NIH HHS/United States
- U10 HL110312/HL/NHLBI NIH HHS/United States
- U01 HL084907/HL/NHLBI NIH HHS/United States
- UL1 TR000135/TR/NCATS NIH HHS/United States
- UL1 TR000454/TR/NCATS NIH HHS/United States
- U10 HL110337/HL/NHLBI NIH HHS/United States
- R01 HL084155/HL/NHLBI NIH HHS/United States
- UL1 RR025008/RR/NCRR NIH HHS/United States
- U10 HL110336/HL/NHLBI NIH HHS/United States
- U10 HL110338/HL/NHLBI NIH HHS/United States
- U01 HL084861/HL/NHLBI NIH HHS/United States
- U10 HL084904/HL/NHLBI NIH HHS/United States
- UL1 TR000439/TR/NCATS NIH HHS/United States
- U10 HL110262/HL/NHLBI NIH HHS/United States
- U10 HL110302/HL/NHLBI NIH HHS/United States
- U10 HL110297/HL/NHLBI NIH HHS/United States
- P01 HL076611/HL/NHLBI NIH HHS/United States
- U01 HL084889/HL/NHLBI NIH HHS/United States
- U10 HL110309/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
