

Analysis of 4000 kidney transplantations in a single center: Across immunological barriers
- PMID: 27512839
- PMCID: PMC4985294
- DOI: 10.1097/MD.0000000000004249
Analysis of 4000 kidney transplantations in a single center: Across immunological barriers
Abstract
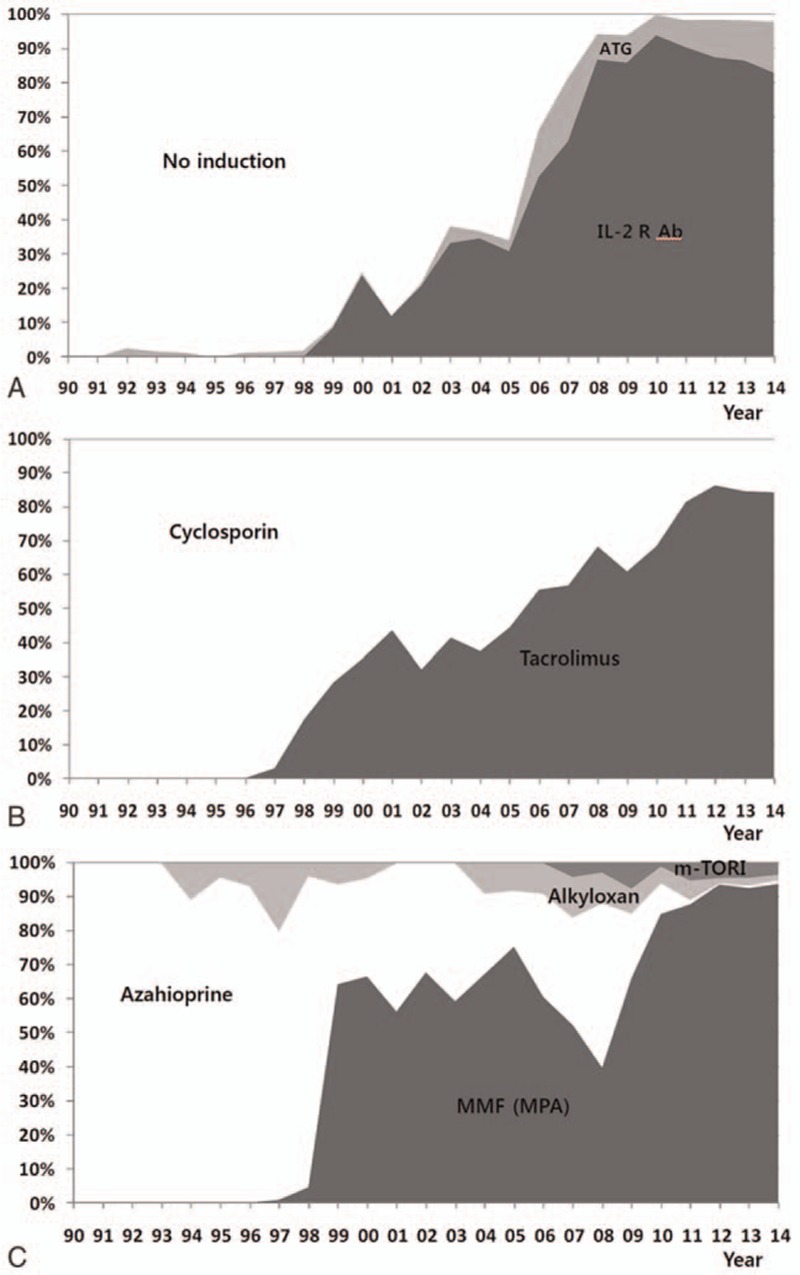
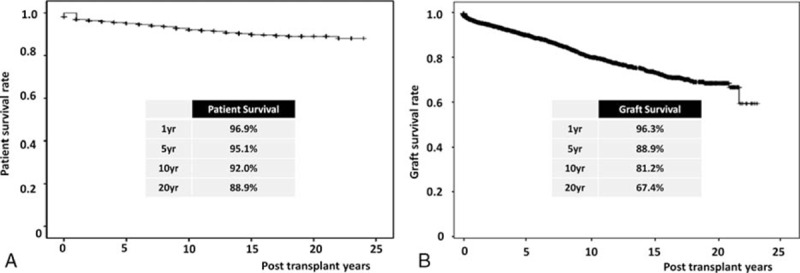
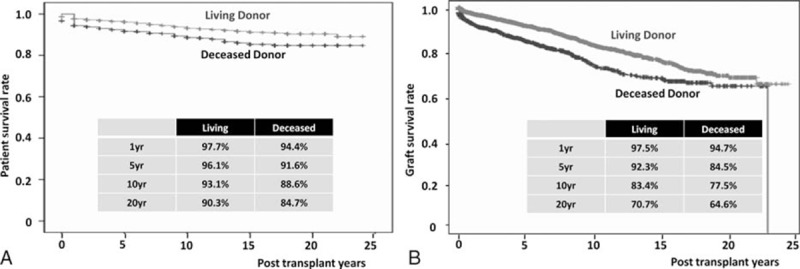
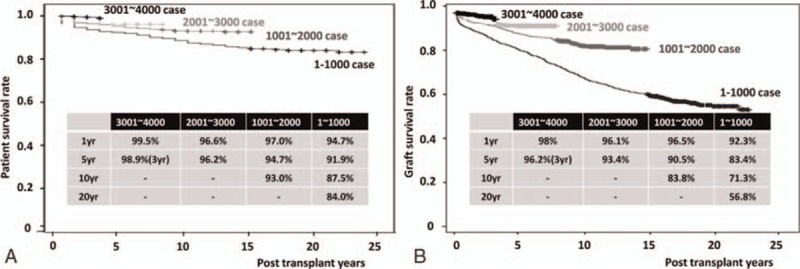
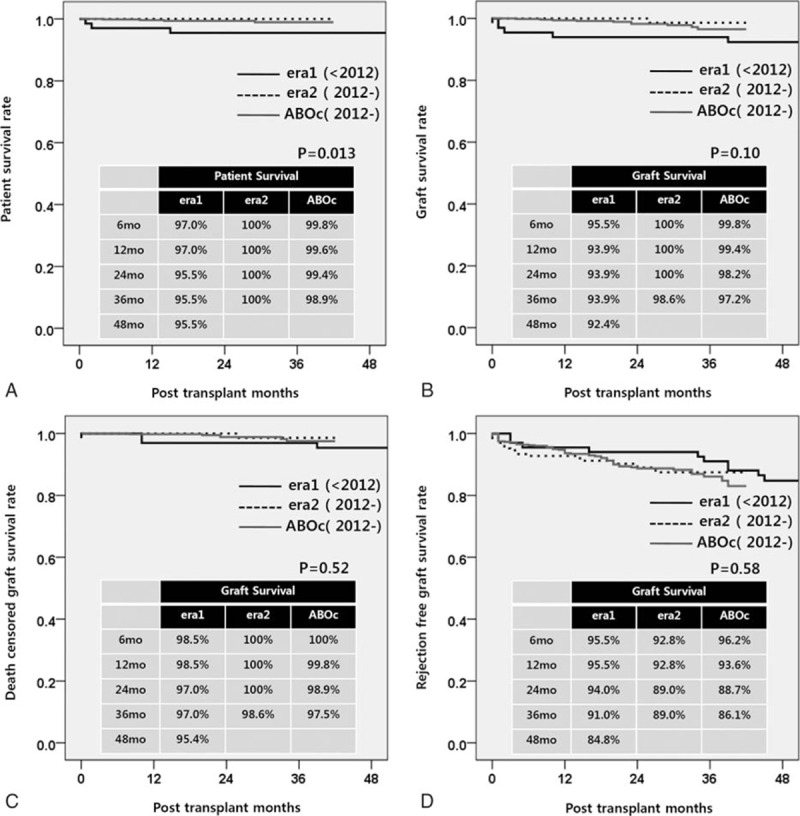
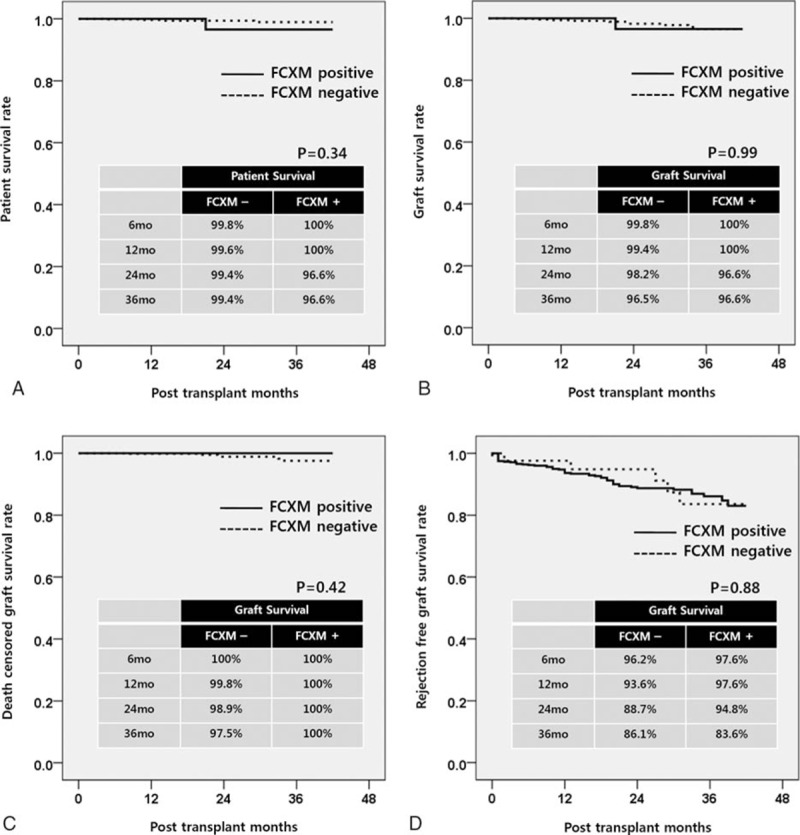
Kidney transplant (KT) is the optimal renal replacement therapy for patients with end-stage renal disease (ESRD). The demand for kidneys, however, continues to exceed the supply. To overcome this problem, efforts to extend the donor pool by including human leukocyte antigen (HLA)- and ABO-incompatible (ABOi) KTs are increasing. The aim of this article was to retrospectively review data on recipients, donor profiles, and clinical outcomes in 4000 cases of KT. In addition, we analyzed clinical outcomes in ABOi and flow-cytometric crossmatch (FCXM) positive KT in a subgroup analysis.This was a retrospective, observational study using data extracted from medical records. A total of 4000 consecutive patients who underwent KT at our institution from January 1990 to February 2015 were included in this study. KTs across immunological barriers such as ABO incompatible (276 cases, 6.9%), FCXM positive (97 cases, 2.4%), and positive complement-dependent cytotoxicity (CDC) XM KT (16 cases, 0.4%) were included.From a Kaplan-Meier analysis, overall patient survival (PS) rates after KT at 1, 5, 10, and 20 years were 96.9%, 95.1%, 92.0%, and 88.9%, respectively. The overall graft survival (GS) rates after KT at 1, 5, 10, and 20 years were 96.3%, 88.9%, 81.2%, and 67.4%, respectively. Our subgroup analysis suggested that overall PS, GS, death-censored GS, and rejection-free GS in ABOi KT showed no significant differences in comparison with ABO-compatible KT if adequate immunosuppressive treatment was performed. The overall PS rate in patients who underwent FCXM positive KT did not differ significantly from that of the control group during the 3-year follow-up (P = 0.34). The overall GS, death-censored GS, and rejection-free GS also did not differ significantly between the FCXM KT and control groups (P = 0.99, 0.42, and 88).The outcomes of KTs continually improved during the study period, while the annual number of KTs increased. ABO or FCXM positive KTs can be performed safely with successful graft outcomes.
Conflict of interest statement
The authors have no funding and conflicts of interest to disclose.
Figures
Similar articles
-
Successful launch of an ABO-incompatible kidney transplantation program to overcome the shortage of compatible living donors: experience at a single center .Clin Nephrol. 2017 Sep;88(9):117-123. doi: 10.5414/CN109114. Clin Nephrol. 2017. PMID: 28679466
-
Acute Rejection and Infectious Complications in ABO- and HLA-Incompatible Kidney Transplantations.Ann Transplant. 2020 Oct 6;25:e927420. doi: 10.12659/AOT.927420. Ann Transplant. 2020. PMID: 33020465 Free PMC article.
-
Transplant outcomes in positive complement-dependent cytotoxicity- versus flow cytometry-crossmatch kidney transplant recipients after successful desensitization: a retrospective study.BMC Nephrol. 2019 Dec 9;20(1):456. doi: 10.1186/s12882-019-1625-2. BMC Nephrol. 2019. PMID: 31818254 Free PMC article.
-
Clinical outcomes after ABO-incompatible renal transplantation: a systematic review and meta-analysis.Lancet. 2019 May 18;393(10185):2059-2072. doi: 10.1016/S0140-6736(18)32091-9. Epub 2019 Apr 18. Lancet. 2019. PMID: 31006573
-
Therapeutic apheresis therapy for ABO-incompatible renal transplantations.Ther Apher Dial. 2003 Dec;7(6):520-8. doi: 10.1046/j.1526-0968.2003.00099.x. Ther Apher Dial. 2003. PMID: 15018238 Review.
Cited by
-
Hepatocellular carcinoma and cancer-related mortality after kidney transplantation with rituximab treatment.Ann Surg Treat Res. 2022 Jan;102(1):55-63. doi: 10.4174/astr.2022.102.1.55. Epub 2022 Jan 3. Ann Surg Treat Res. 2022. PMID: 35071120 Free PMC article.
-
Rituximab protects against development of atherosclerotic cardiovascular disease after kidney transplantation: a propensity-matched study.Sci Rep. 2019 Nov 11;9(1):16475. doi: 10.1038/s41598-019-52942-8. Sci Rep. 2019. PMID: 31712593 Free PMC article.
-
Effect of simultaneous presence of anti-blood group A/B and -HLA antibodies on clinical outcomes in kidney transplantation across positive crossmatch: a nationwide cohort study.Sci Rep. 2019 Dec 3;9(1):18229. doi: 10.1038/s41598-019-54397-3. Sci Rep. 2019. PMID: 31796812 Free PMC article.
-
Effect of arteriovenous access closure and timing on kidney function in kidney transplant recipients.PLoS One. 2019 Dec 11;14(12):e0226309. doi: 10.1371/journal.pone.0226309. eCollection 2019. PLoS One. 2019. PMID: 31826011 Free PMC article.
-
Polyomavirus Nephropathy in ABO Blood Group-Incompatible Kidney Transplantation: Torque Teno Virus and Immunosuppressive Burden as an Approximation to the Problem.Kidney Int Rep. 2024 Apr 3;9(6):1730-1741. doi: 10.1016/j.ekir.2024.04.003. eCollection 2024 Jun. Kidney Int Rep. 2024. PMID: 38899213 Free PMC article.
References
-
- Wolfe RA, Ashby VB, Milford EL, et al. Comparison of mortality in all patients on dialysis, patients on dialysis awaiting transplantation, and recipients of a first cadaveric transplant. N Engl J Med 1999; 341:1725–1730. - PubMed
-
- Korean Network for Organ Sharing (KONOS). (internet)URL: http://www.cdc.go.kr/CDC/contents/CdcKrContentLink.jsp?fid=3081&cid=2427....
-
- Shrestha B, Haylor J, Raftery A. Historical perspectives in kidney transplantation: an updated review. Prog Transplant 2015; 25:64–69. - PubMed
-
- Shin S, Kim YH, Choi BH, et al. Long-term impact of human leukocyte antigen mismatches combined with expanded criteria donor on allograft outcomes in deceased donor kidney transplantation. Clin Transplant 2015; 29:44–51. - PubMed
-
- Opelz G, Morath C, Susal C, et al. Three-year outcomes following 1420 ABO-incompatible living-donor kidney transplants performed after ABO antibody reduction: results from 101 centers. Transplantation 2015; 99:400–404. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
