

Zero-fluoroscopy catheter ablation of severe drug-resistant arrhythmia guided by Ensite NavX system during pregnancy: Two case reports and literature review
- PMID: 27512864
- PMCID: PMC4985319
- DOI: 10.1097/MD.0000000000004487
Zero-fluoroscopy catheter ablation of severe drug-resistant arrhythmia guided by Ensite NavX system during pregnancy: Two case reports and literature review
Abstract
Background: Cardiac arrhythmias can occur during pregnancy. Owing to radiation exposure and other uncertain risks for the mother and fetus, catheter ablation has rarely been performed and is often delayed until the postpartum period. We reported 2 pregnant women who were experiencing severe arrhythmias and were successfully ablated without fluoroscopic guidance. We also carried out a literature review of cases of pregnant women who underwent zero-fluoroscopy ablation.
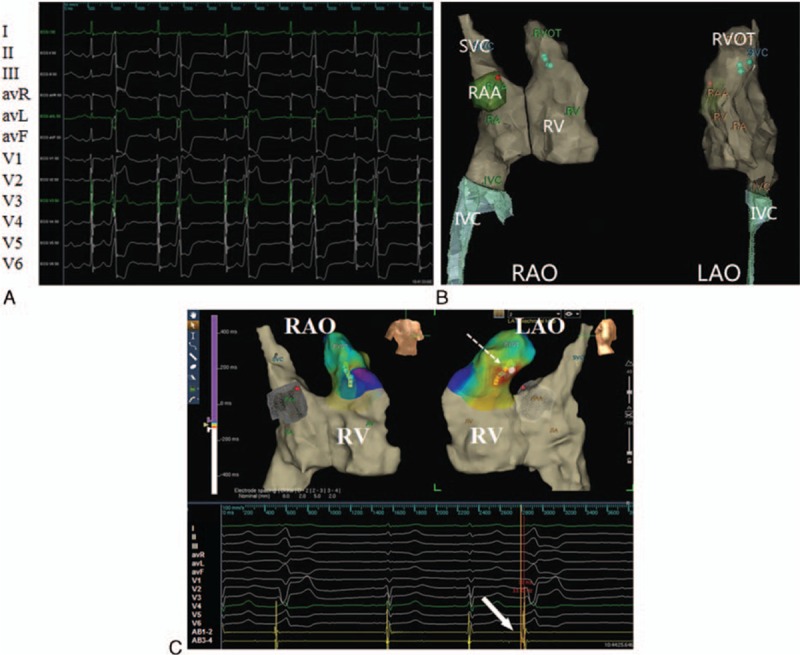
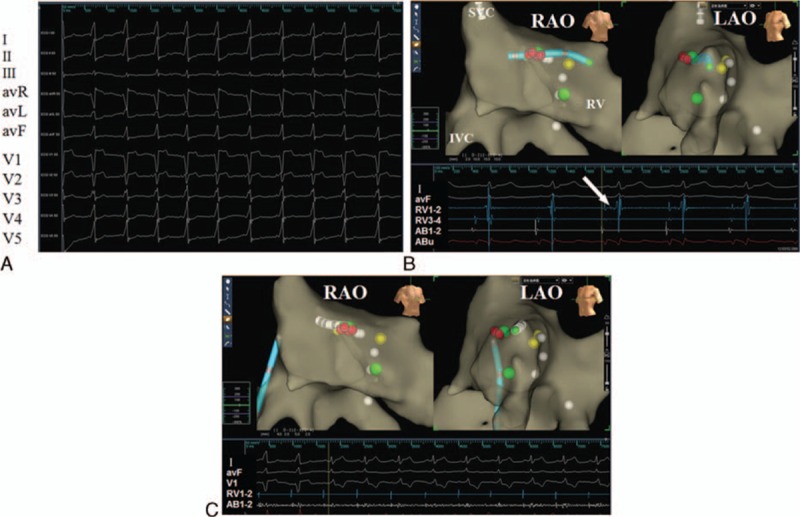
Methods and results: One woman had drug-resistant and poorly tolerated frequent premature ventricular contraction (PVC) and ventricular tachycardia (VT). The other one had persistent and hardly terminated supraventricular tachycardia (SVT) via a right accessory pathway. The 2 patients were successfully underwent zero-fluoroscopy ablation guided by Ensite NavX system. The procedure time was 42 and 71 minutes, respectively.
Conclusion: Catheter ablation of SVT or PVC/VT in pregnant patients can be safely and effectively performed with a completely zero-fluoroscopy approach guided by the Ensite NavX system. In the case of a drug refractory, life-threatening arrhythmia during pregnancy, catheter ablation may be considered.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
Similar articles
-
Zero-fluoroscopy approach for ablation of supraventricular tachycardia using the Ensite NavX system: a multicenter experience.BMC Cardiovasc Disord. 2020 Feb 3;20(1):48. doi: 10.1186/s12872-020-01344-0. BMC Cardiovasc Disord. 2020. PMID: 32013865 Free PMC article.
-
[Radiofrequency catheter ablation of arrhythmias in pediatric patients guided by three-dimensional mapping system].Zhonghua Er Ke Za Zhi. 2009 Sep;47(9):705-9. Zhonghua Er Ke Za Zhi. 2009. PMID: 20021797 Chinese.
-
Emergent Zero-Fluoroscopy Mapping and Thoracoscopic Ectomy of Appendage in Pregnant Women with Life-Threatening Atrial Tachycardia: A Case Report and Literature Review.Medicina (Kaunas). 2023 Mar 8;59(3):528. doi: 10.3390/medicina59030528. Medicina (Kaunas). 2023. PMID: 36984528 Free PMC article. Review.
-
Radiofrequency ablation of arrhythmias guided by non-fluoroscopic catheter location: a prospective randomized trial.Eur Heart J. 2006 May;27(10):1223-9. doi: 10.1093/eurheartj/ehi834. Epub 2006 Apr 13. Eur Heart J. 2006. PMID: 16613932 Clinical Trial.
-
Comparison of minimal versus zero-fluoroscopic catheter ablation in gestational supraventricular arrhythmias.J Interv Card Electrophysiol. 2023 Sep;66(6):1423-1429. doi: 10.1007/s10840-022-01444-1. Epub 2022 Dec 10. J Interv Card Electrophysiol. 2023. PMID: 36495414 Review.
Cited by
-
Feasibility and performance of catheter ablation with zero-fluoroscopy approach for regular supraventricular tachycardia in patients with structural and/or congenital heart disease.Medicine (Baltimore). 2019 Oct;98(41):e17333. doi: 10.1097/MD.0000000000017333. Medicine (Baltimore). 2019. PMID: 31593082 Free PMC article.
-
Zero-fluoroscopy approach for ablation of supraventricular tachycardia using the Ensite NavX system: a multicenter experience.BMC Cardiovasc Disord. 2020 Feb 3;20(1):48. doi: 10.1186/s12872-020-01344-0. BMC Cardiovasc Disord. 2020. PMID: 32013865 Free PMC article.
-
Ablation of idiopathic ventricular arrhythmia using zero-fluoroscopy approach with equivalent efficacy and less fatigue: A multicenter comparative study.Medicine (Baltimore). 2017 Feb;96(6):e6080. doi: 10.1097/MD.0000000000006080. Medicine (Baltimore). 2017. PMID: 28178165 Free PMC article.
-
Intracardiac echocardiography Chinese expert consensus.Front Cardiovasc Med. 2022 Oct 6;9:1012731. doi: 10.3389/fcvm.2022.1012731. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 36277762 Free PMC article. Review.
-
The Fluoroless Future in Electrophysiology: A State-of-the-Art Review.Diagnostics (Basel). 2024 Jan 14;14(2):182. doi: 10.3390/diagnostics14020182. Diagnostics (Basel). 2024. PMID: 38248058 Free PMC article. Review.
References
-
- Moore JS, Teefey P, Rao K, et al. Maternal arrhythmia: a case report and review of the literature. Obstet Gynecol Surv 2012; 67:298–312. - PubMed
-
- Robins K, Lyons G. Supraventricular tachycardia in pregnancy. Br J Anaesth 2004; 92:140–143. - PubMed
-
- Knotts RJ, Garan H. Cardiac arrhythmias in pregnancy. Semin Perinatol 2014; 38:285–288. - PubMed
-
- Bigelow AM, Crane SS, Khoury FR, et al. Catheter ablation of supraventricular tachycardia without fluoroscopy during pregnancy. Obstet Gynecol 2015; 125:1338–1341. - PubMed
-
- McAnulty JH. Arrhythmias in pregnancy. Cardiol Clin 2012; 30:425–434. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
