

Pediatric Sepsis Biomarker Risk Model-II: Redefining the Pediatric Sepsis Biomarker Risk Model With Septic Shock Phenotype
- PMID: 27513537
- PMCID: PMC5201138
- DOI: 10.1097/CCM.0000000000001852
Pediatric Sepsis Biomarker Risk Model-II: Redefining the Pediatric Sepsis Biomarker Risk Model With Septic Shock Phenotype
Abstract
Objective: The Pediatric Sepsis Biomarker Risk Model (PERSEVERE), a pediatric sepsis risk model, uses biomarkers to estimate baseline mortality risk for pediatric septic shock. It is unknown how PERSEVERE performs within distinct septic shock phenotypes. We tested PERSEVERE in children with septic shock and thrombocytopenia-associated multiple organ failure (TAMOF), and in those without new onset thrombocytopenia but with multiple organ failure (MOF).
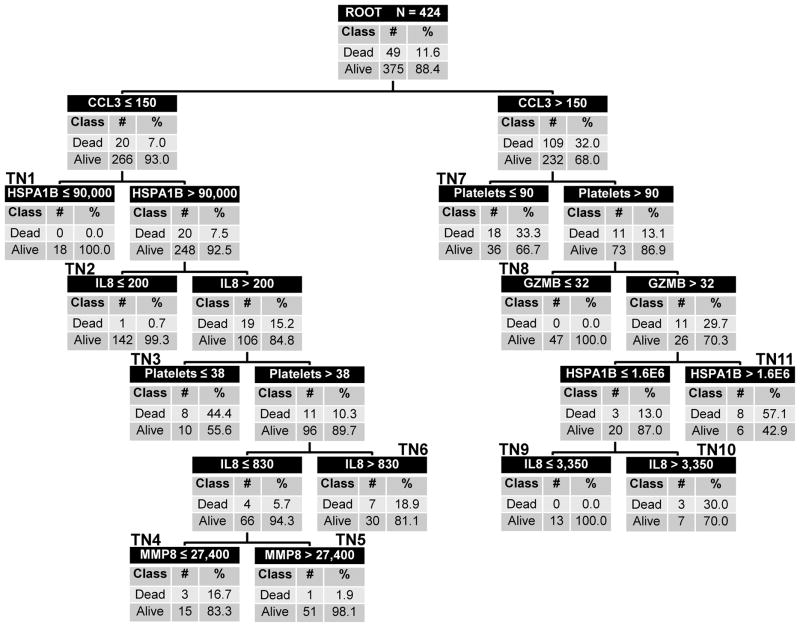
Design: PERSEVERE-based mortality risk was generated for each study subject (n = 660). A priori, we determined that if PERSEVERE did not perform well in both the TAMOF and the MOF cohorts, we would revise PERSEVERE to incorporate admission platelet counts.
Setting: Multiple PICUs in the United States.
Interventions: Standard care.
Measurements and main results: PERSEVERE performed well in the TAMOF cohort (areas under the receiver operating characteristic curves [AUC], 0.84 [95% CI, 0.77-0.90]), but less well in the MOF cohort (AUC, 0.71 [0.61-0.80]). PERSEVERE was revised using 424 subjects previously reported in the derivation phase. PERSEVERE-II had an AUC of 0.89 (0.85-0.93) and performed equally well across TAMOF and MOF cohorts. PERSEVERE-II performed well when tested in 236 newly enrolled subjects. Sample size calculations for a clinical trial testing the efficacy of plasma exchange for children with septic shock and TAMOF indicated PERSEVERE-II-based stratification could substantially reduce the number of patients necessary, when compared with no stratification.
Conclusions: Testing PERSEVERE in the context of septic shock phenotypes prompted a revision incorporating platelet count. PERSEVERE-II performs well upon testing, independent of TAMOF or MOF status. PERSEVERE-II could potentially serve as a prognostic enrichment tool.
Conflict of interest statement
AUTHOR COMPETING INTERESTS Dr. Wong and the Cincinnati Children’s Hospital Research Foundation have submitted a provisional patent application for PERSEVERE. Dr. Lindsell is named as a co-inventor in the above patent application. The other authors have no competing interests to report.
Figures
References
-
- Cohen J, Vincent JL, Adhikari NK, Machado FR, Angus DC, Calandra T, Jaton K, Giulieri S, Delaloye J, Opal S, et al. Sepsis: a roadmap for future research. Lancet Infect Dis. 2015;15(5):581–614. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
