

Long-Term Training with a Brain-Machine Interface-Based Gait Protocol Induces Partial Neurological Recovery in Paraplegic Patients
- PMID: 27513629
- PMCID: PMC4980986
- DOI: 10.1038/srep30383
Long-Term Training with a Brain-Machine Interface-Based Gait Protocol Induces Partial Neurological Recovery in Paraplegic Patients
Abstract
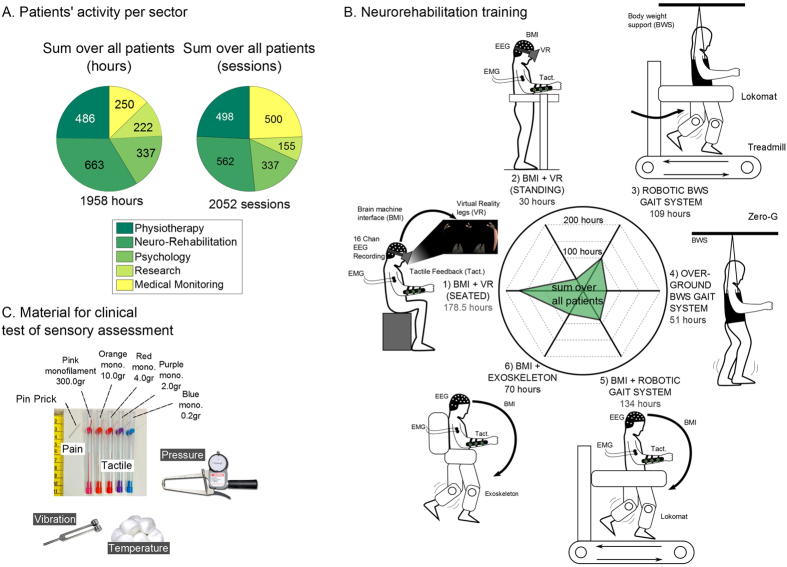
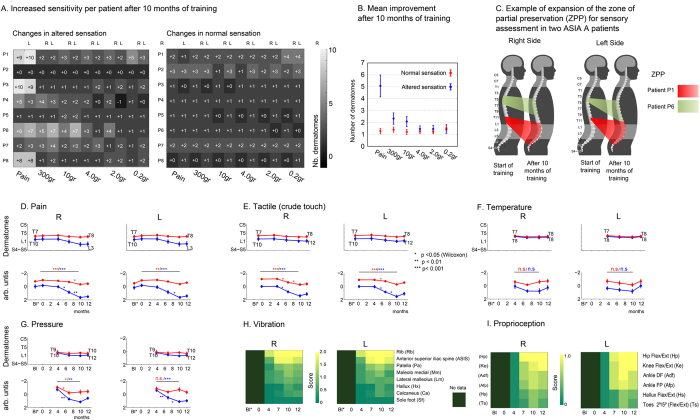
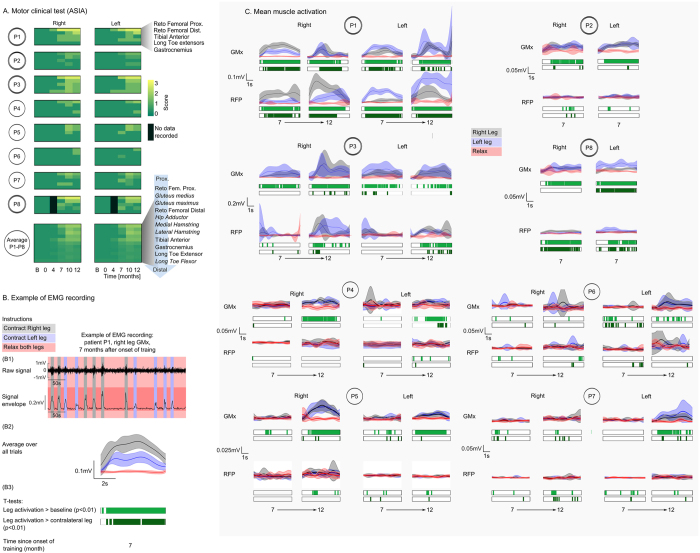
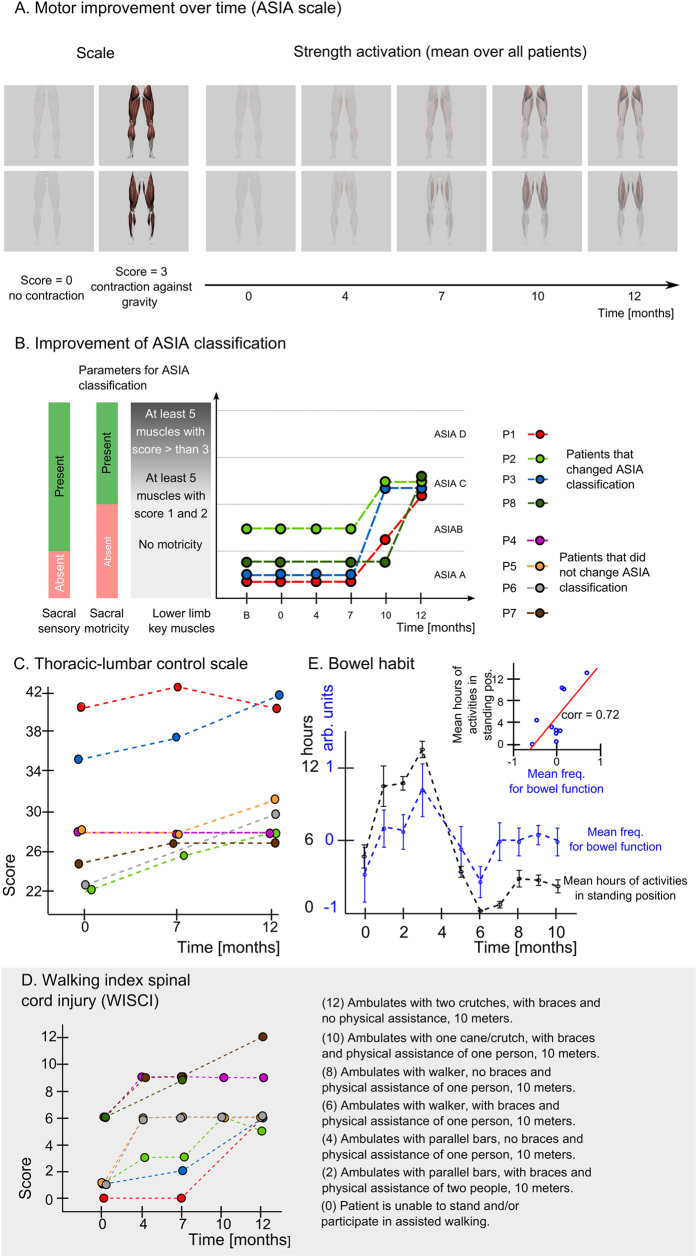
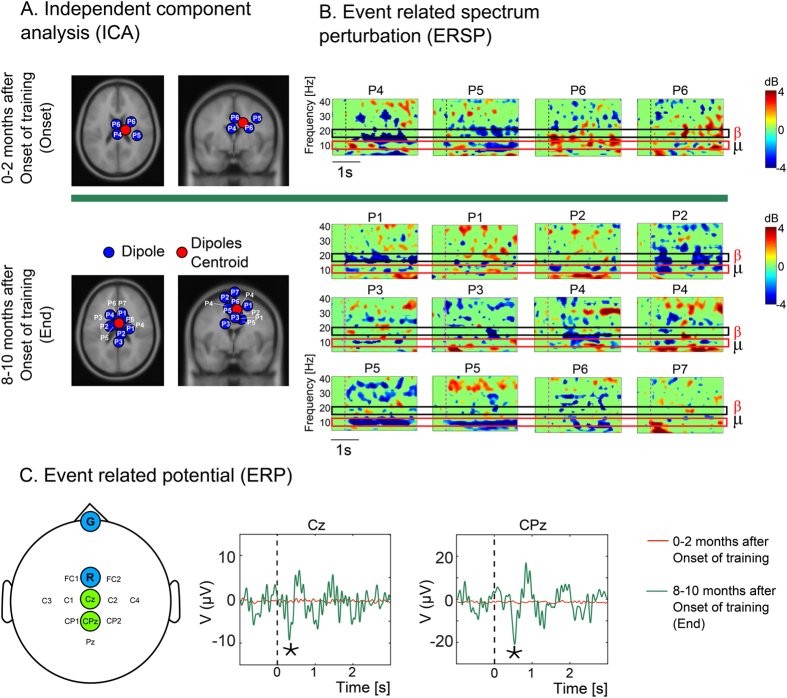
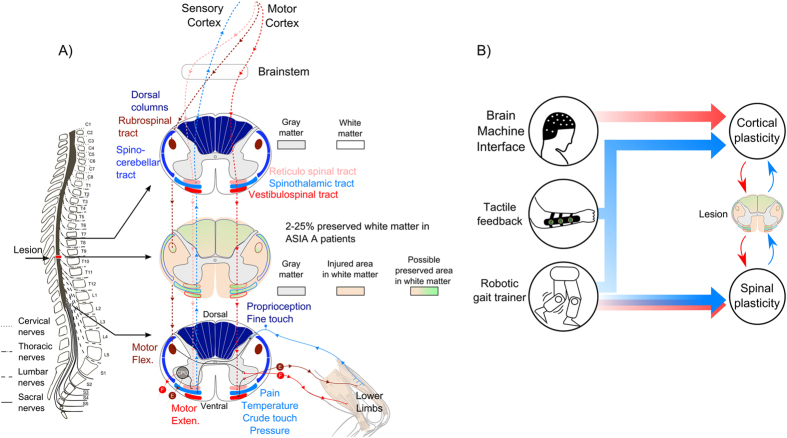
Brain-machine interfaces (BMIs) provide a new assistive strategy aimed at restoring mobility in severely paralyzed patients. Yet, no study in animals or in human subjects has indicated that long-term BMI training could induce any type of clinical recovery. Eight chronic (3-13 years) spinal cord injury (SCI) paraplegics were subjected to long-term training (12 months) with a multi-stage BMI-based gait neurorehabilitation paradigm aimed at restoring locomotion. This paradigm combined intense immersive virtual reality training, enriched visual-tactile feedback, and walking with two EEG-controlled robotic actuators, including a custom-designed lower limb exoskeleton capable of delivering tactile feedback to subjects. Following 12 months of training with this paradigm, all eight patients experienced neurological improvements in somatic sensation (pain localization, fine/crude touch, and proprioceptive sensing) in multiple dermatomes. Patients also regained voluntary motor control in key muscles below the SCI level, as measured by EMGs, resulting in marked improvement in their walking index. As a result, 50% of these patients were upgraded to an incomplete paraplegia classification. Neurological recovery was paralleled by the reemergence of lower limb motor imagery at cortical level. We hypothesize that this unprecedented neurological recovery results from both cortical and spinal cord plasticity triggered by long-term BMI usage.
Figures
Comment in
-
Long-term Training With a Brain-Machine Interface-Based Gait Protocol Induces Partial Neurological Recovery in Paraplegic Patients.Neurosurgery. 2016 Dec;79(6):N13-N14. doi: 10.1227/01.neu.0000508601.15824.39. Neurosurgery. 2016. PMID: 27861407 No abstract available.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
