

Imaging biomarkers for steatohepatitis and fibrosis detection in non-alcoholic fatty liver disease
- PMID: 27514671
- PMCID: PMC4981860
- DOI: 10.1038/srep31421
Imaging biomarkers for steatohepatitis and fibrosis detection in non-alcoholic fatty liver disease
Abstract
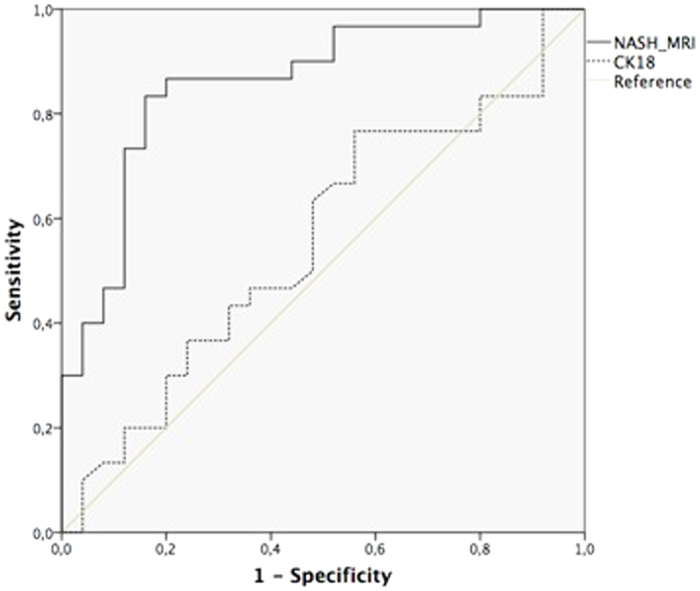
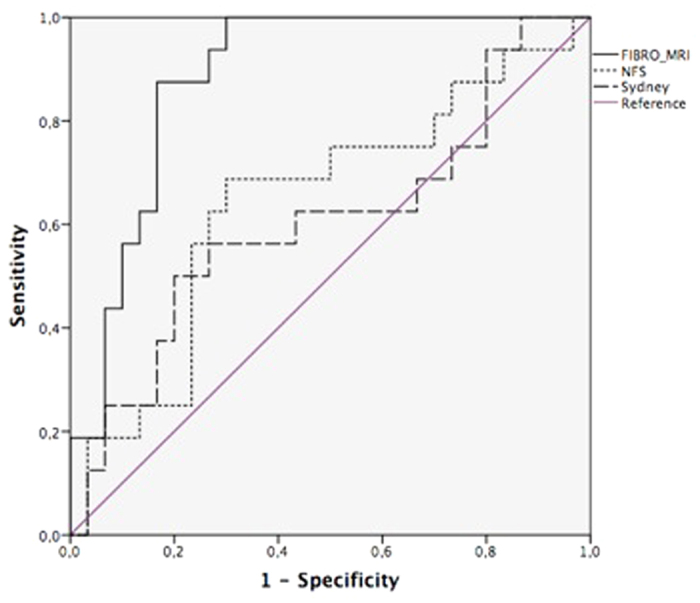
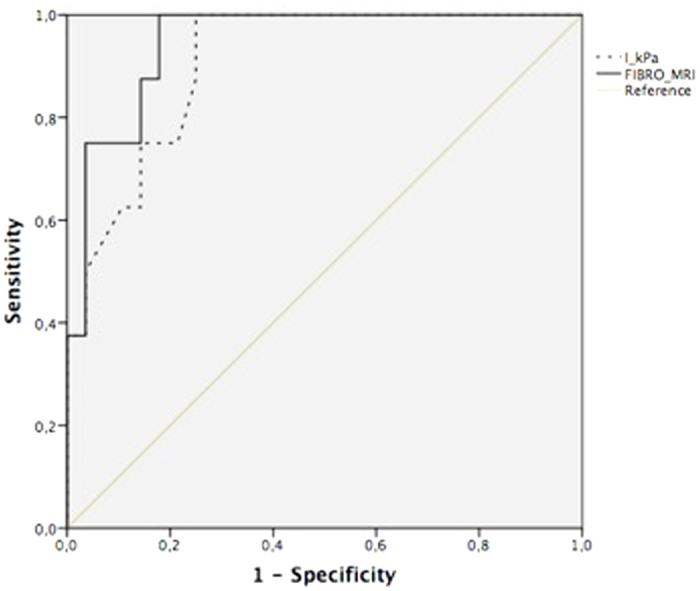
There is a need, in NAFLD management, to develop non-invasive methods to detect steatohepatitis (NASH) and to predict advanced fibrosis stages. We evaluated a tool based on optical analysis of liver magnetic resonance images (MRI) as biomarkers for NASH and fibrosis detection by investigating patients with biopsy-proven NAFLD who underwent magnetic resonance (MR) protocols using 1.5T General Electric (GE) or Philips devices. Two imaging biomarkers (NASHMRI and FibroMRI) were developed, standardised and validated using area under the receiver operating characteristic curve (AUROC) analysis. The results indicated NASHMRI diagnostic accuracy for steatohepatitis detection was 0.83 (95% CI: 0.73-0.93) and FibroMRI diagnostic accuracy for significant fibrosis determination was 0.85 (95% CI: 0.77-0.94). These findings were independent of the MR system used. We conclude that optical analysis of MRI has high potential to define non-invasive imaging biomarkers for the detection of steatohepatitis (NASHMRI) and the prediction of significant fibrosis (FibroMRI) in NAFLD patients.
Figures
References
-
- Chalasani N. et al. The diagnosis and management of non-alcoholic fatty liver disease: practice guideline by the American Gastroenterological Association, American Association for the Study of Liver Diseases, and American College of Gastroenterology. Gastroenterology 142, 1592–1609 (2012). - PubMed
-
- Wong V. W. et al. Prevalence of non-alcoholic fatty liver disease and advanced fibrosis in Hong Kong Chinese: a population study using proton-magnetic resonance spectroscopy and transient elastography. Gut 2012 61, 409–415 (2012). - PubMed
-
- Bellentani S. & Marino M. Epidemiology and natural history of non-alcoholic fatty liver disease (NAFLD). Ann. Hepatol. 8, S4–S8 (2009). - PubMed
-
- affy G., Brunt E. M. & Caldwell S. H. Hepatocellular carcinoma in non-alcoholic fatty liver disease: an emerging menace. J. Hepatol. 56, 1384–1391 (2012). - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
