

Mortality and transmissibility patterns of the 1957 influenza pandemic in Maricopa County, Arizona
- PMID: 27516082
- PMCID: PMC4982429
- DOI: 10.1186/s12879-016-1716-7
Mortality and transmissibility patterns of the 1957 influenza pandemic in Maricopa County, Arizona
Abstract
Background: While prior studies have quantified the mortality burden of the 1957 H2N2 influenza pandemic at broad geographic regions in the United States, little is known about the pandemic impact at a local level. Here we focus on analyzing the transmissibility and mortality burden of this pandemic in Arizona, a setting where the dry climate was promoted as reducing respiratory illness transmission yet tuberculosis prevalence was high.
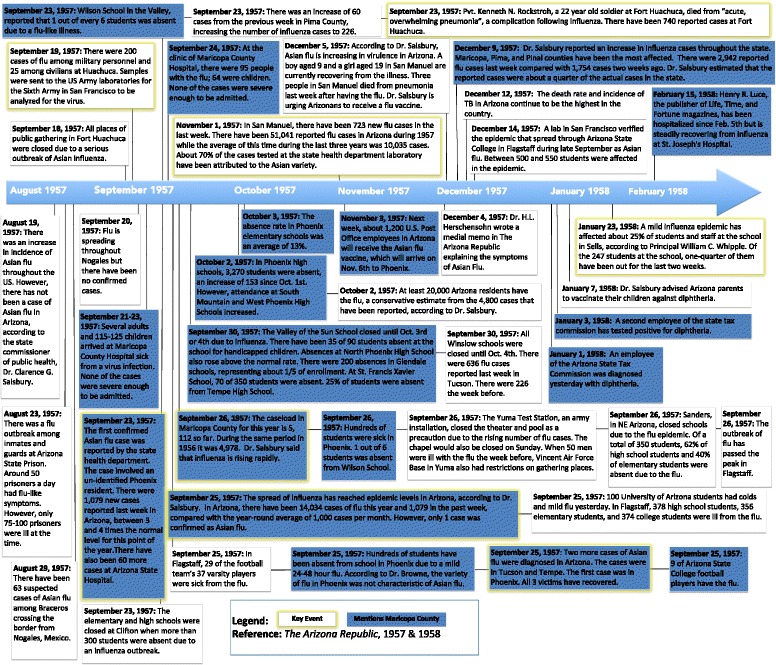
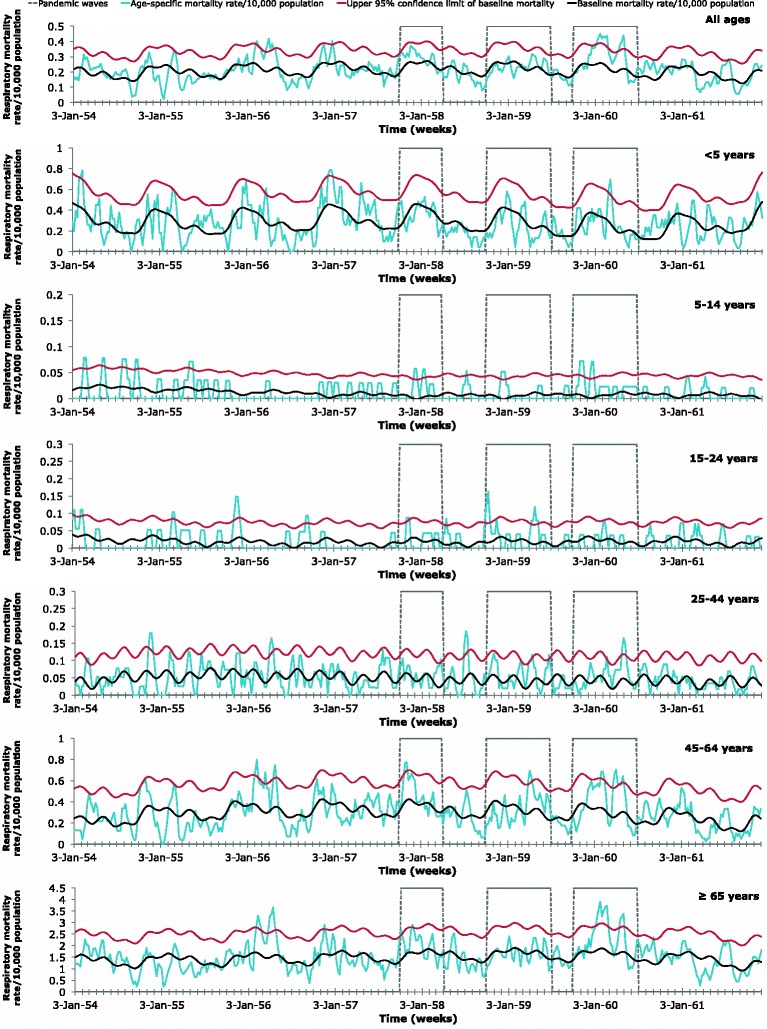
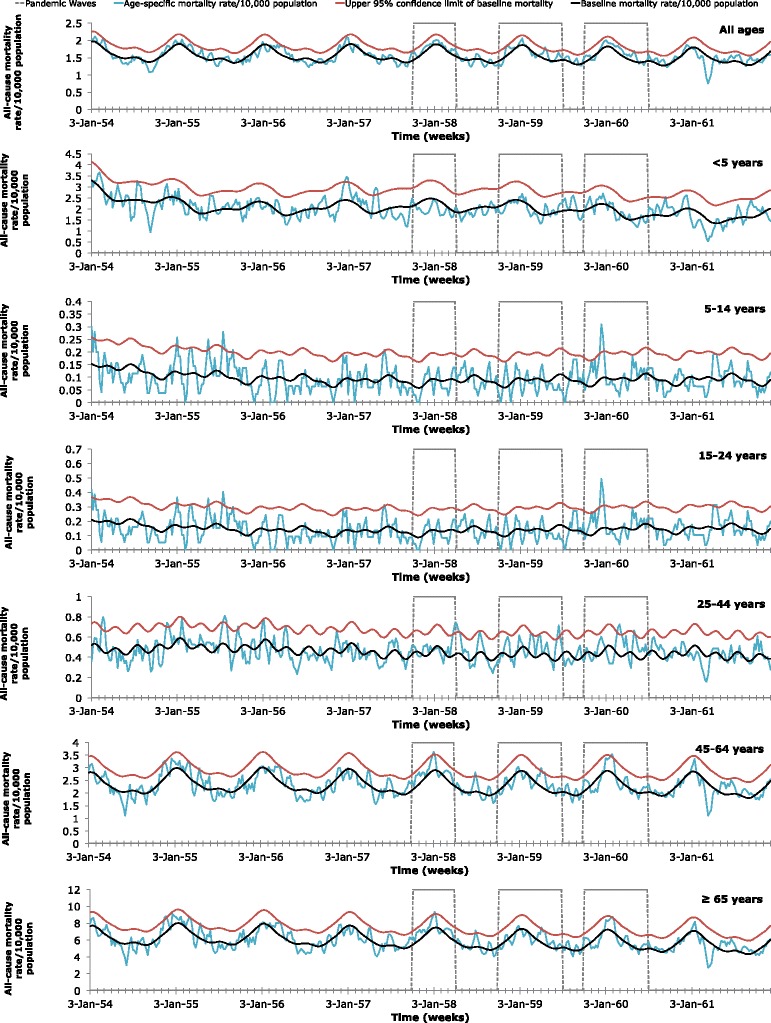
Methods: Using archival death certificates from 1954 to 1961, we quantified the age-specific seasonal patterns, excess-mortality rates, and transmissibility patterns of the 1957 H2N2 pandemic in Maricopa County, Arizona. By applying cyclical Serfling linear regression models to weekly mortality rates, the excess-mortality rates due to respiratory and all-causes were estimated for each age group during the pandemic period. The reproduction number was quantified from weekly data using a simple growth rate method and assumed generation intervals of 3 and 4 days. Local newspaper articles published during 1957-1958 were also examined.
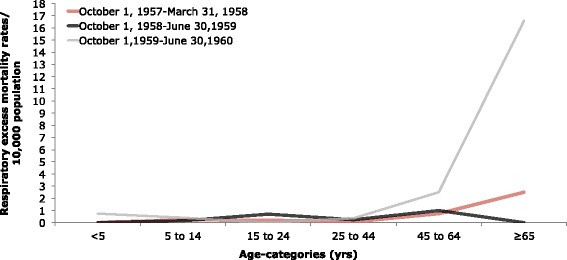
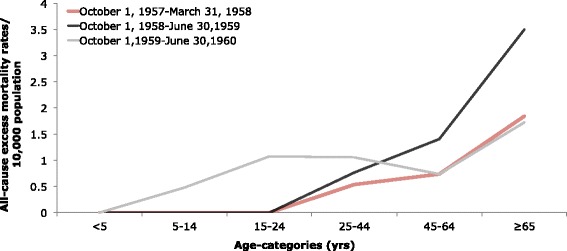
Results: Excess-mortality rates varied between waves, age groups, and causes of death, but overall remained low. From October 1959-June 1960, the most severe wave of the pandemic, the absolute excess-mortality rate based on respiratory deaths per 10,000 population was 16.59 in the elderly (≥65 years). All other age groups exhibit very low excess-mortality and the typical U-shaped age-pattern was absent. However, the standardized mortality ratio was greatest (4.06) among children and young adolescents (5-14 years) from October 1957-March 1958, based on mortality rates of respiratory deaths. Transmissibility was greatest during the same 1957-1958 period, when the mean reproduction number was estimated at 1.08-1.11, assuming 3- or 4-day generation intervals with exponential or fixed distributions.
Conclusions: Maricopa County exhibited very low mortality impact associated with the 1957 influenza pandemic. Understanding the relatively low excess-mortality rates and transmissibility in Maricopa County during this historic pandemic may help public health officials prepare for and mitigate future outbreaks of influenza.
Keywords: 1957 influenza; Arizona; Asian influenza; H2N2 virus; Maricopa County; Mathematical epidemiology; Mortality rates; Reproduction number; Transmissibility.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
