

Morphofunctional Abnormalities of Mitral Annulus and Arrhythmic Mitral Valve Prolapse
- PMID: 27516479
- PMCID: PMC4991345
- DOI: 10.1161/CIRCIMAGING.116.005030
Morphofunctional Abnormalities of Mitral Annulus and Arrhythmic Mitral Valve Prolapse
Abstract
Background: Arrhythmic mitral valve prolapse (MVP) is characterized by myxomatous leaflets and left ventricular (LV) fibrosis of papillary muscles and inferobasal wall. We searched for morphofunctional abnormalities of the mitral valve that could explain a regional mechanical myocardial stretch.
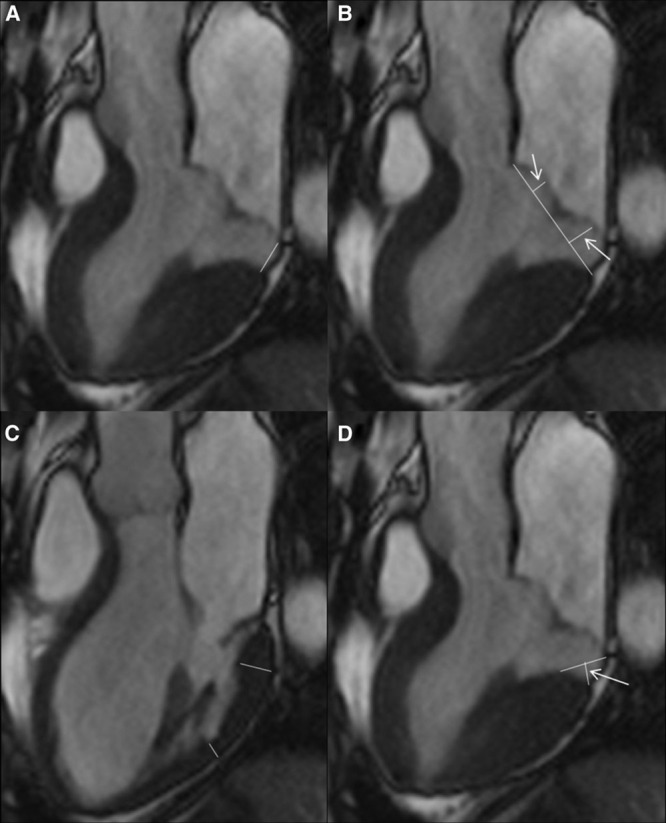
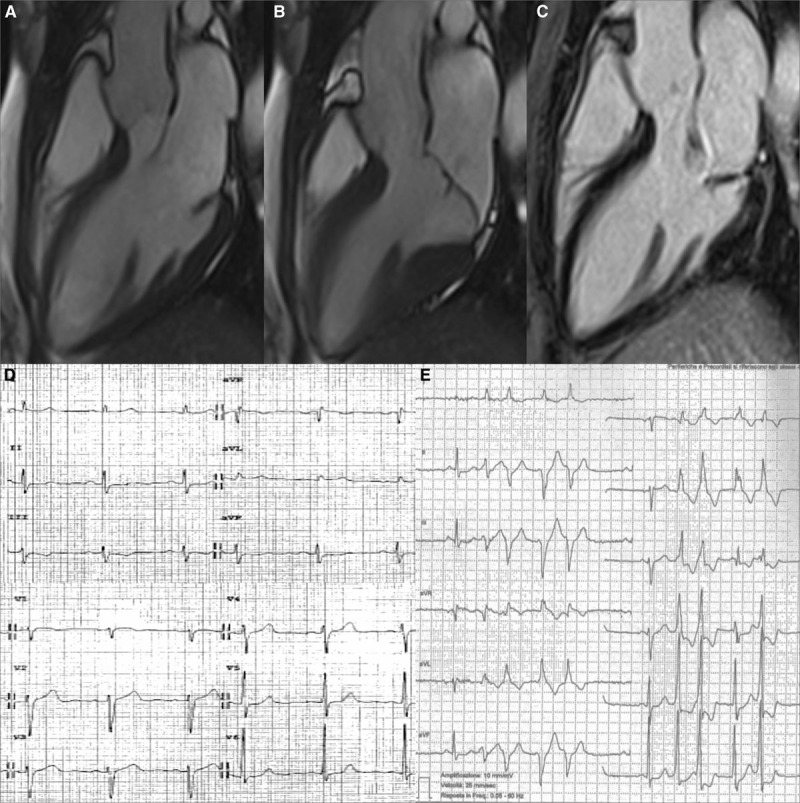
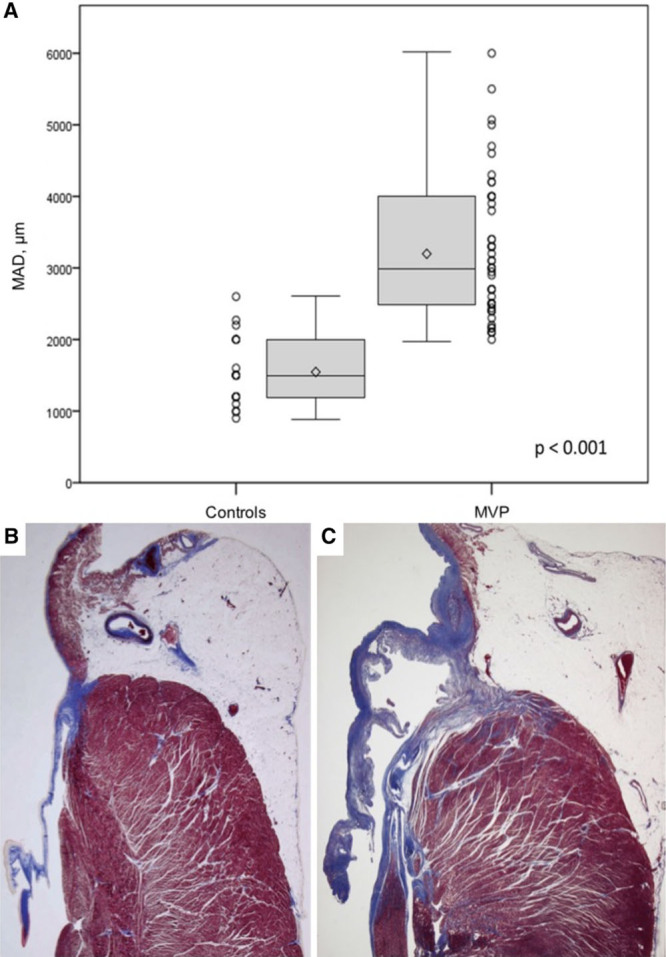
Methods and results: Thirty-six (27 female patients; median age: 44 years) arrhythmic MVP patients with LV late gadolinium enhancement on cardiac magnetic resonance and no or trivial mitral regurgitation, and 16 (6 female patients; median age: 40 years) MVP patients without LV late gadolinium enhancement were investigated by morphofunctional cardiac magnetic resonance. Mitral annulus disjunction (median: 4.8 versus 1.8 mm; P<0.001), end-systolic mitral annular diameters (median: 41.2 versus 31.5; P=0.004) and end-diastolic mitral annular diameters (median: 35.5 versus 31.5; P=0.042), prevalence of posterior systolic curling (34 [94%] versus 3 [19%]; P<0.001), and basal to mid LV wall thickness ratio >1.5 (22 [61%] versus 4 [25%]; P=0.016) were higher in MVP patients with late gadolinium enhancement than in those without. A linear correlation was found between mitral annulus disjunction and curling (R=0.85). A higher prevalence of auscultatory midsystolic click (26 [72%] versus 6 [38%]; P=0.018) was also noted. Histology of the mitral annulus showed a longer mitral annulus disjunction in 50 sudden death patients with MVP and LV fibrosis than in 20 patients without MVP (median: 3 versus 1.5 mm; P<0.001).
Conclusions: Mitral annulus disjunction is a constant feature of arrhythmic MVP with LV fibrosis. The excessive mobility of the leaflets caused by posterior systolic curling accounts for a mechanical stretch of the inferobasal wall and papillary muscles, eventually leading to myocardial hypertrophy and scarring. These mitral annulus abnormalities, together with auscultatory midsystolic click, may identify MVP patients who would need arrhythmic risk stratification.
Keywords: gadolinium; mitral valve; mitral valve annulus; mitral valve prolapse; papillary muscles.
© 2016 The Authors.
Figures


Comment in
-
Malignant Mitral Valve Prolapse: Substrates to Ventricular Remodeling and Arrhythmias.Circ Cardiovasc Imaging. 2016 Aug;9(8):e005248. doi: 10.1161/CIRCIMAGING.116.005248. Circ Cardiovasc Imaging. 2016. PMID: 27516480 No abstract available.
References
-
- Basso C, Perazzolo Marra M, Rizzo S, De Lazzari M, Giorgi B, Cipriani A, Frigo AC, Rigato I, Migliore F, Pilichou K, Bertaglia E, Cacciavillani L, Bauce B, Corrado D, Thiene G, Iliceto S. Arrhythmic mitral valve prolapse and sudden cardiac death. Circulation. 2015;132:556–566. doi: 10.1161/CIRCULATIONAHA.115.016291. - PubMed
-
- Hutchins GM, Moore GW, Skoog DK. The association of floppy mitral valve with disjunction of the mitral annulus fibrosus. N Engl J Med. 1986;314:535–540. doi: 10.1056/NEJM198602273140902. - PubMed
-
- Eriksson MJ, Bitkover CY, Omran AS, David TE, Ivanov J, Ali MJ, Woo A, Siu SC, Rakowski H. Mitral annular disjunction in advanced myxomatous mitral valve disease: echocardiographic detection and surgical correction. J Am Soc Echocardiogr. 2005;18:1014–1022. doi: 10.1016/j.echo.2005.06.013. - PubMed
-
- Weis AJ, Salcedo EE, Stewart WJ, Lever HM, Klein AL, Thomas JD. Anatomic explanation of mobile systolic clicks: implications for the clinical and echocardiographic diagnosis of mitral valve prolapse. Am Heart J. 1995;129:314–320. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
