

A Sound Therapy-Based Intervention to Expand the Auditory Dynamic Range for Loudness among Persons with Sensorineural Hearing Losses: A Randomized Placebo-Controlled Clinical Trial
- PMID: 27516711
- PMCID: PMC4906300
- DOI: 10.1055/s-0035-1546958
A Sound Therapy-Based Intervention to Expand the Auditory Dynamic Range for Loudness among Persons with Sensorineural Hearing Losses: A Randomized Placebo-Controlled Clinical Trial
Abstract
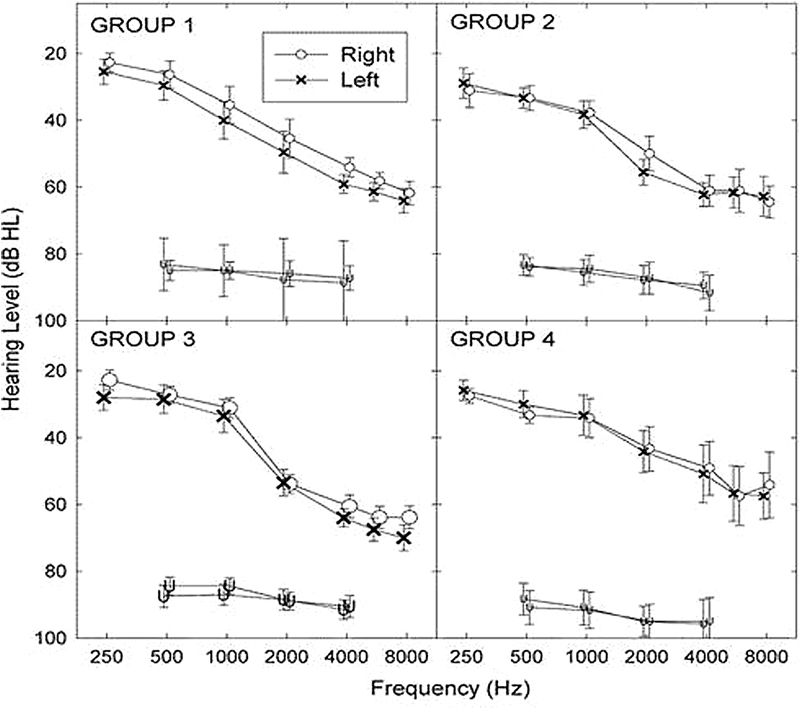
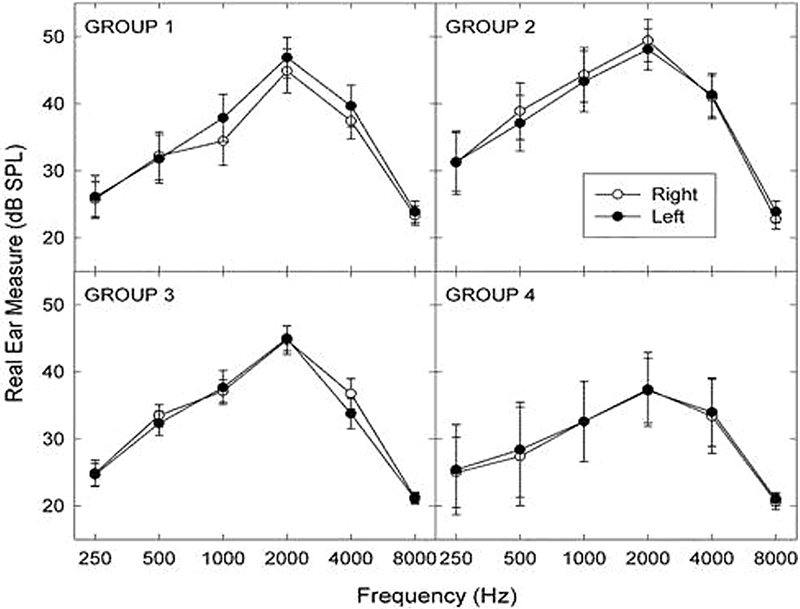
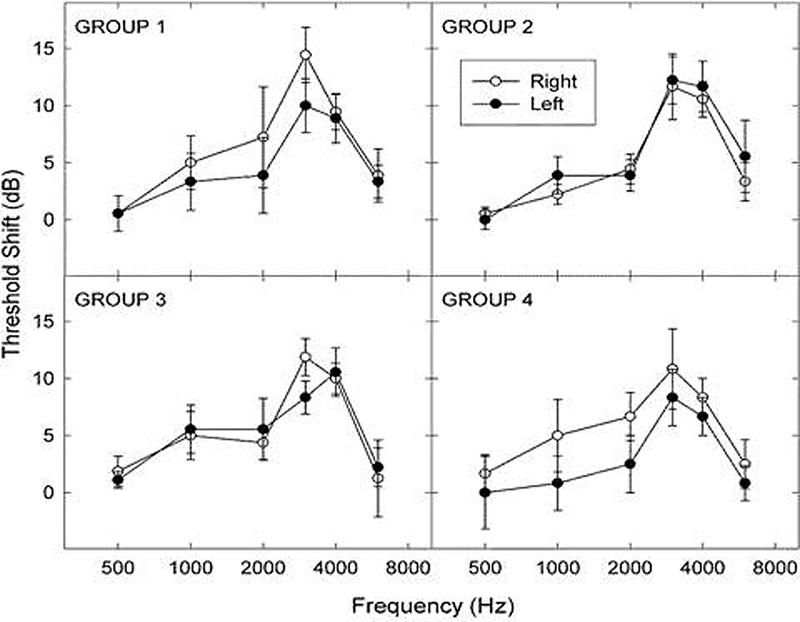
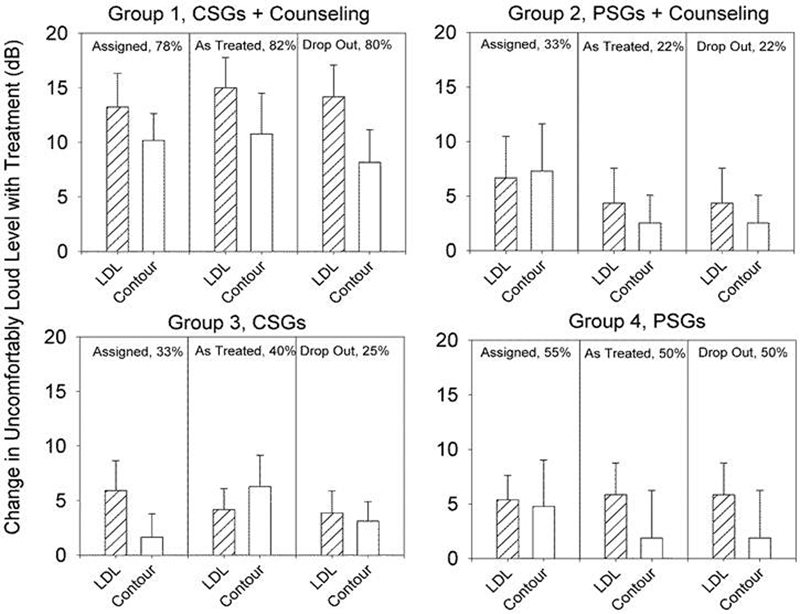
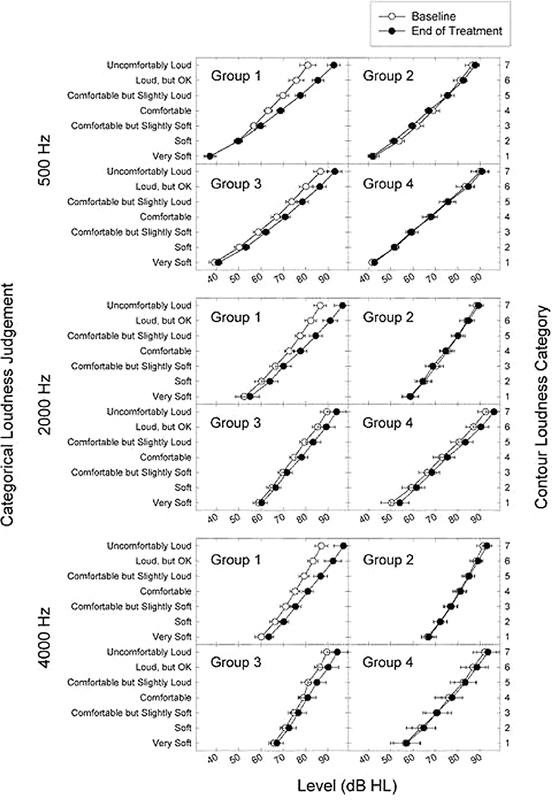
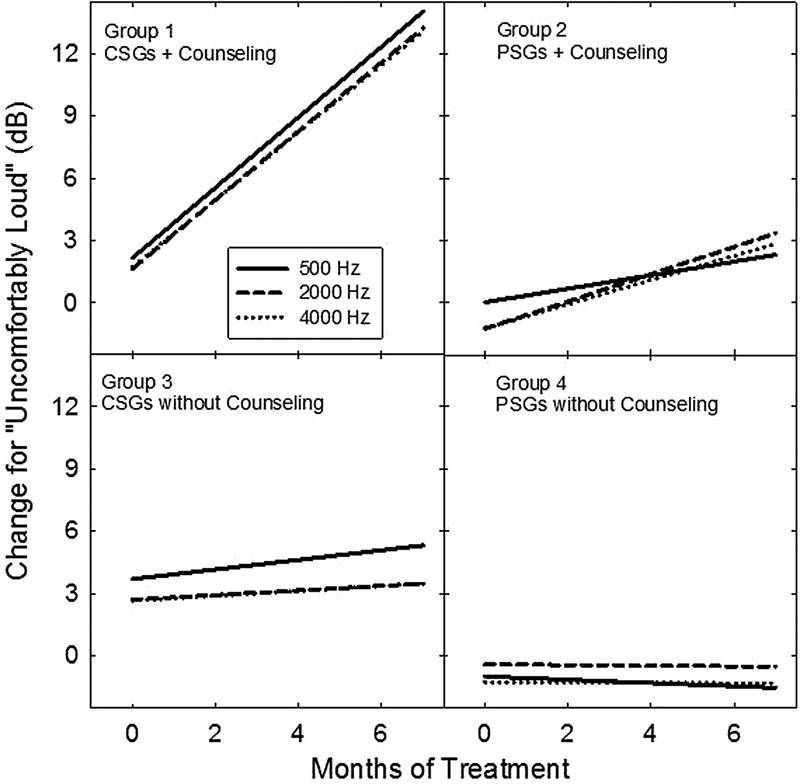
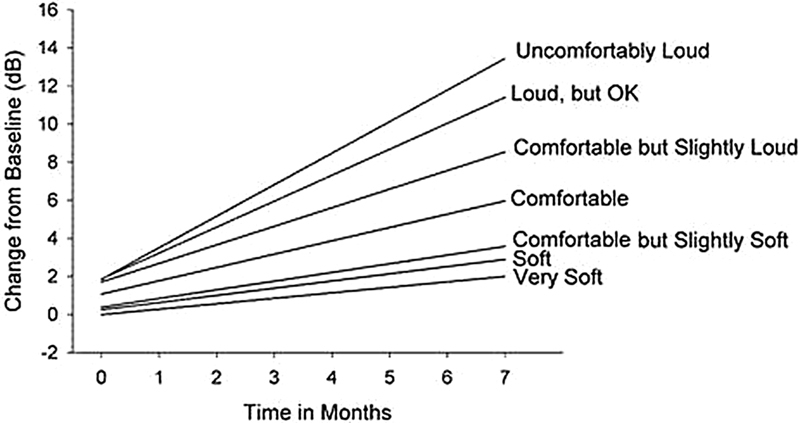
The primary aim of this research was to evaluate the validity, efficacy, and generalization of principles underlying a sound therapy-based treatment for promoting expansion of the auditory dynamic range (DR) for loudness. The basic sound therapy principles, originally devised for treatment of hyperacusis among patients with tinnitus, were evaluated in this study in a target sample of unsuccessfully fit and/or problematic prospective hearing aid users with diminished DRs (owing to their elevated audiometric thresholds and reduced sound tolerance). Secondary aims included: (1) delineation of the treatment contributions from the counseling and sound therapy components to the full-treatment protocol and, in turn, the isolated treatment effects from each of these individual components to intervention success; and (2) characterization of the respective dynamics for full, partial, and control treatments. Thirty-six participants with bilateral sensorineural hearing losses and reduced DRs, which affected their actual or perceived ability to use hearing aids, were enrolled in and completed a placebo-controlled (for sound therapy) randomized clinical trial. The 2 × 2 factorial trial design was implemented with or without various assignments of counseling and sound therapy. Specifically, participants were assigned randomly to one of four treatment groups (nine participants per group), including: (1) group 1-full treatment achieved with scripted counseling plus sound therapy implemented with binaural sound generators; (2) group 2-partial treatment achieved with counseling and placebo sound generators (PSGs); (3) group 3-partial treatment achieved with binaural sound generators alone; and (4) group 4-a neutral control treatment implemented with the PSGs alone. Repeated measurements of categorical loudness judgments served as the primary outcome measure. The full-treatment categorical-loudness judgments for group 1, measured at treatment termination, were significantly greater than the corresponding pretreatment judgments measured at baseline at 500, 2,000, and 4,000 Hz. Moreover, increases in their "uncomfortably loud" judgments (∼12 dB over the range from 500 to 4,000 Hz) were superior to those measured for either of the partial-treatment groups 2 and 3 or for control group 4. Efficacy, assessed by treatment-related criterion increases ≥ 10 dB for judgments of uncomfortable loudness, was superior for full treatment (82% efficacy) compared with that for either of the partial treatments (25% and 40% for counseling combined with the placebo sound therapy and sound therapy alone, respectively) or for the control treatment (50%). The majority of the group 1 participants achieved their criterion improvements within 3 months of beginning treatment. The treatment effect from sound therapy was much greater than that for counseling, which was statistically indistinguishable in most of our analyses from the control treatment. The basic principles underlying the full-treatment protocol are valid and have general applicability for expanding the DR among individuals with sensorineural hearing losses, who may often report aided loudness problems. The positive full-treatment effects were superior to those achieved for either counseling or sound therapy in virtual or actual isolation, respectively; however, the delivery of both components in the full-treatment approach was essential for an optimum treatment outcome.
Keywords: Sound tolerance; hyperacusis; loudness discomfort level; sound therapy.
Figures


Similar articles
-
Structured Counseling for Auditory Dynamic Range Expansion.Semin Hear. 2017 Feb;38(1):115-129. doi: 10.1055/s-0037-1598068. Semin Hear. 2017. PMID: 28286367 Free PMC article. Review.
-
Auditory Brainstem and Middle Latency Responses Measured Pre- and Posttreatment for Hyperacusic Hearing-Impaired Persons Successfully Treated to Improve Sound Tolerance and to Expand the Dynamic Range for Loudness: Case Evidence.Semin Hear. 2017 Feb;38(1):71-93. doi: 10.1055/s-0037-1598066. Semin Hear. 2017. PMID: 28286365 Free PMC article. Review.
-
A Sound Therapy-Based Intervention to Expand the Auditory Dynamic Range for Loudness among Persons with Sensorineural Hearing Losses: Case Evidence Showcasing Treatment Efficacy.Semin Hear. 2017 Feb;38(1):130-150. doi: 10.1055/s-0037-1598069. Semin Hear. 2017. PMID: 28286368 Free PMC article. Review.
-
Repeated Measurement of Absolute and Relative Judgments of Loudness: Clinical Relevance for Prescriptive Fitting of Aided Target Gains for soft, Comfortable, and Loud, But Ok Sound Levels.Semin Hear. 2017 Feb;38(1):26-52. doi: 10.1055/s-0037-1598064. Semin Hear. 2017. PMID: 28286363 Free PMC article. Review.
-
Results of a 6-Month Field Trial of a Transitional Intervention for Debilitating Hyperacusis.J Speech Lang Hear Res. 2024 Jun 6;67(6):1903-1931. doi: 10.1044/2024_JSLHR-23-00360. Epub 2024 May 8. J Speech Lang Hear Res. 2024. PMID: 38718263 Free PMC article. Clinical Trial.
Cited by
-
Functional magnetic resonance imaging of enhanced central auditory gain and electrophysiological correlates in a behavioral model of hyperacusis.Hear Res. 2020 Apr;389:107908. doi: 10.1016/j.heares.2020.107908. Epub 2020 Feb 6. Hear Res. 2020. PMID: 32062293 Free PMC article.
-
Considerations in the Development of a Sound Tolerance Interview and Questionnaire Instrument.Semin Hear. 2017 Feb;38(1):53-70. doi: 10.1055/s-0037-1598065. Semin Hear. 2017. PMID: 28286364 Free PMC article. Review.
-
Clinical Interventions for Hyperacusis in Adults: A Scoping Review to Assess the Current Position and Determine Priorities for Research.Biomed Res Int. 2017;2017:2723715. doi: 10.1155/2017/2723715. Epub 2017 Oct 9. Biomed Res Int. 2017. PMID: 29312994 Free PMC article.
-
Current Recommendations for the Use of Sound Therapy in Adults with Hyperacusis: A Scoping Review.Brain Sci. 2024 Aug 9;14(8):797. doi: 10.3390/brainsci14080797. Brain Sci. 2024. PMID: 39199489 Free PMC article.
-
Bilateral versus unilateral hearing aids for bilateral hearing impairment in adults.Cochrane Database Syst Rev. 2017 Dec 19;12(12):CD012665. doi: 10.1002/14651858.CD012665.pub2. Cochrane Database Syst Rev. 2017. PMID: 29256573 Free PMC article.
References
-
- Hazell J WP Sheldrake J B Hyperacusis and tinnitus In: Aran J M Dauman R, eds. . Tinnitus 91. Proceedings of the Fourth International Tinnitus Seminar Amsterdam/New York: Kugler Publications; 1992245–248.
-
- Jastreboff P J, Hazell J WP. A neurophysiological approach to tinnitus: clinical implications. Br J Audiol. 1993;27(1):7–17. - PubMed
-
- Jastreboff P J, Gray W C, Gold S L. Neurophysiological approach to tinnitus patients. Am J Otol. 1996;17(2):236–240. - PubMed
-
- Jastreboff P J, Hazell J. Cambridge, UK: Cambridge University Press; 2004. Tinnitus Retraining Therapy: Implementing the Neurophysiological Model.
-
- Jastreboff P J, Jastreboff M M. Tinnitus Retraining Therapy (TRT) as a method for treatment of tinnitus and hyperacusis patients. J Am Acad Audiol. 2000;11(3):162–177. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
