

An updated systematic review and meta-analysis on the efficacy and tolerability of dipeptidyl peptidase-4 inhibitors in patients with type 2 diabetes with moderate to severe chronic kidney disease
- PMID: 27516879
- PMCID: PMC4968114
- DOI: 10.1177/2050312116659090
An updated systematic review and meta-analysis on the efficacy and tolerability of dipeptidyl peptidase-4 inhibitors in patients with type 2 diabetes with moderate to severe chronic kidney disease
Abstract
Objective: This updated meta-analysis determines the effect of dipeptidyl peptidase-4 inhibitors on glycemic and tolerability outcomes in patients with type 2 diabetes mellitus and chronic kidney disease with glomerular filtration rate of ⩽60 mL/min or on dialysis.
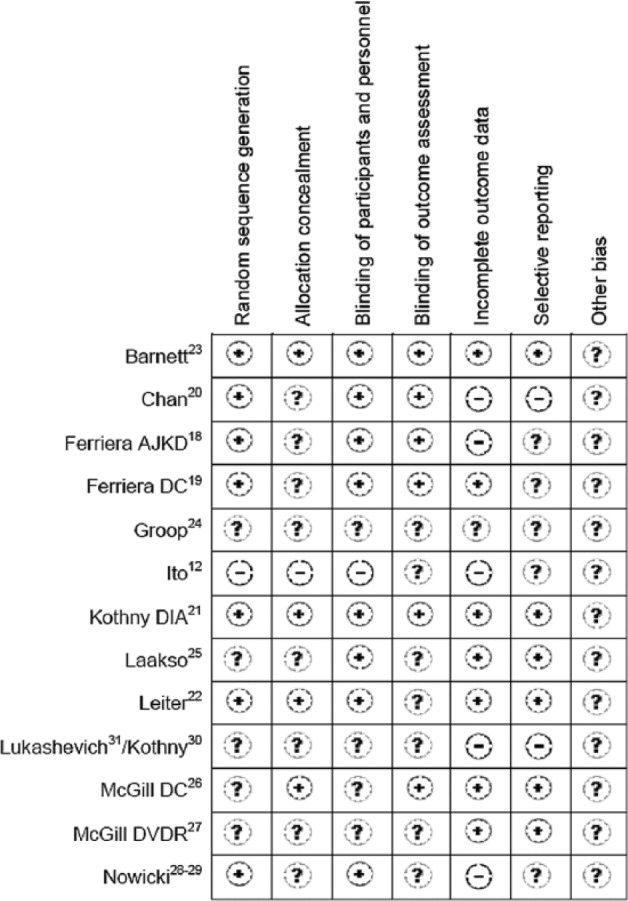
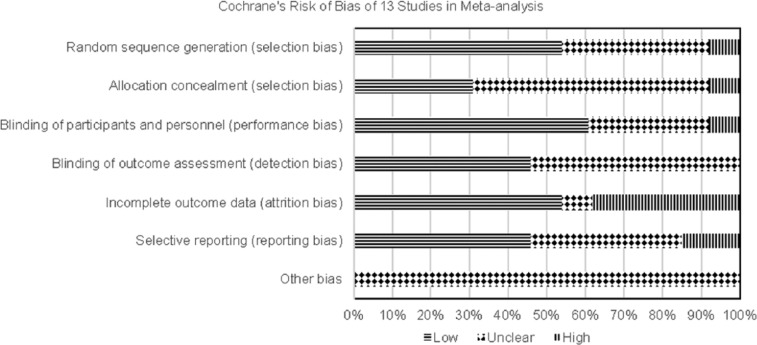
Methods: In all, 14 citations were identified from multiple databases. Qualitative assessments and quantitative analyses were performed.
Results: There were 2261 participants, 49-79 years of age, 49% men and 44% Caucasians. In seven placebo-comparator studies, reduction in hemoglobin A1c at weeks 12-24 was 0.55% (95% confidence interval: -0.68 to -0.43), P < 0.00001). In three sulfonylurea-comparator studies, dipeptidyl peptidase-4 inhibitors did not significantly reduce hemoglobin A1c at weeks 52-54 (-0.15% (95% confidence interval: -0.32 to 0.02)). In one sitagliptin versus albiglutide study, albiglutide significantly reduced hemoglobin A1c in patients with moderate renal impairment (-0.51%). A similar reduction in hemoglobin A1c was seen with sitagliptin versus vildagliptin (-0.56% vs -0.54%). Compared with placebo or sulfonylurea, dipeptidyl peptidase-4 inhibitors did not significantly reduce hemoglobin A1c after 12 and 54 weeks in patients on dialysis. Hypoglycemia was reported by ~30% of patients in both dipeptidyl peptidase-4 inhibitors and placebo groups over 24-52 weeks. While hypoglycemia was more common with a sulfonylurea at 52-54 weeks (risk ratio: 0.46 (95% confidence interval: 0.18 to 1.18)), there was significant heterogeneity (I (2) = 87%). Limitations included high drop-out rate from most studies and small number of active-comparator studies.
Conclusions: Dipeptidyl peptidase-4 inhibitors in patients with chronic kidney disease caused a modest reduction in hemoglobin A1c versus placebo, but not when compared with sulfonylureas or albiglutide, or when used in patients on dialysis. Additional active-comparator studies are needed to further elucidate the role of dipeptidyl peptidase-4 inhibitors in patients with chronic kidney disease stages 3-5 or on dialysis.
Keywords: Meta-analysis; chronic kidney disease; dialysis; dipeptidyl peptidase-4 inhibitors; linagliptin; saxagliptin; sitagliptin; type 2 diabetes mellitus; vildagliptin.
Conflict of interest statement
Figures





References
-
- KDIGO CKD Work Group. KDIGO 2012 clinical practice guideline for the evaluation of chronic kidney disease. Kidney Int 2013; 3: 1–150. - PubMed
-
- American Diabetes Association. Microvascular complications and foot care. Diabetes Care 2016; 39(Suppl. 1): S72–S80. - PubMed
-
- National Diabetes Statistics Report, 2014. Estimates of diabetes and its burden in the United States, http://www.cdc.gov/diabetes/pubs/statsreport14/national-diabetes-report-... (accessed 19 October 2015).
-
- US Renal Data System. USRDS 2013 annual data report: atlas of chronic kidney disease and end-stage renal disease in the United States. Bethesda, MD: National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases, 2013.
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
