

What's new in the functional anatomy of pelvic organ prolapse?
- PMID: 27517338
- PMCID: PMC5347042
- DOI: 10.1097/GCO.0000000000000312
What's new in the functional anatomy of pelvic organ prolapse?
Abstract
Purpose of review: Provide an evidence-based review of pelvic floor functional anatomy related to pelvic organ prolapse.
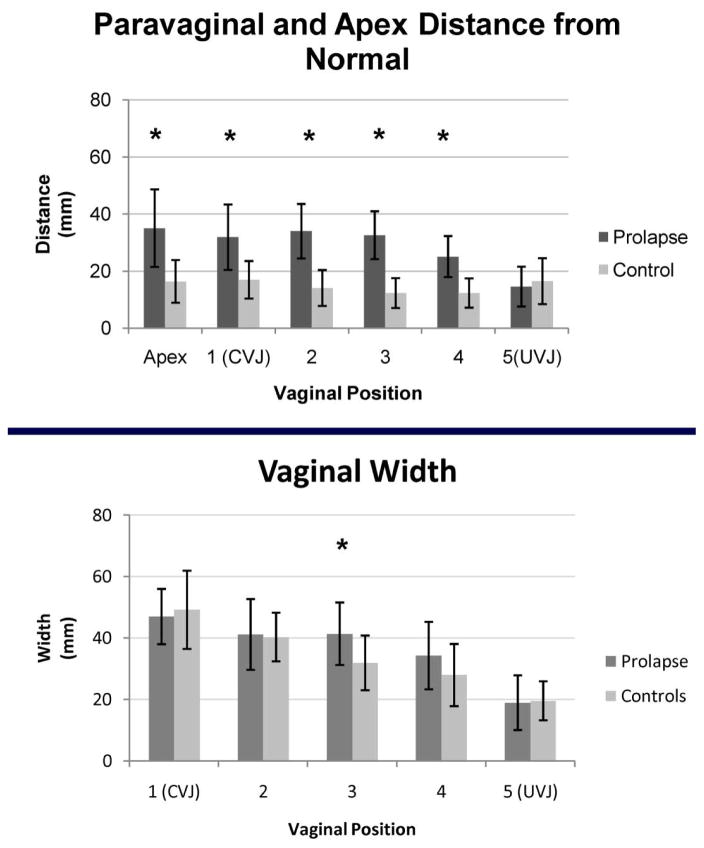
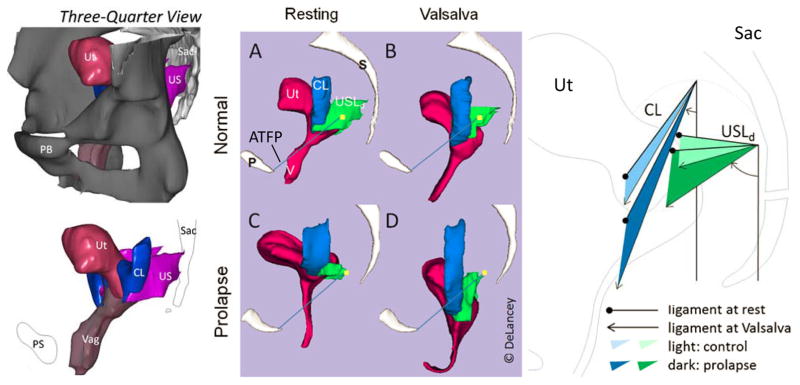
Recent findings: Pelvic organ support depends on interactions between the levator ani muscle and pelvic connective tissues. Muscle failure exposes the vaginal wall to a pressure differential producing abnormal tension on the attachments of the pelvic organs to the pelvic sidewall. Birth-induced injury to the pubococcygeal portion of the levator ani muscle is seen in 55% of women with prolapse and 16% of women with normal support. Failure of the lateral connective tissue attachments between the uterus and vagina to the pelvic wall (cardinal, uterosacral, and paravaginal) are strongly related with prolapse (effect sizes ∼2.5) and are also highly correlated with one another (r ∼ 0.85). Small differences exist with prolapse in factors involving the vaginal wall length and width (effect sizes ∼1). The primary difference in ligament properties between women with and without prolapse is found in ligament length. Only minor differences in ligament stiffness are seen.
Summary: Pelvic organ prolapse occurs because of injury to the levator ani muscles and failure of the lateral connections between the pelvic organs to the pelvic sidewall. Abnormalities of the vaginal wall fascial tissues may play a minor role.
Conflict of interest statement
Conflicts of interest: None.
Figures





References
-
- Delancey JO. Surgery for cystocele III: do all cystoceles involve apical descent?: Observations on cause and effect. International urogynecology journal. 2012;23:665–7. This article describes a conceptual understanding about the basic mechanisms of cystocele formation that includes the interaction between apical support and muscle function. - PubMed
-
- Rubod C, Lecomte-Grosbras P, Brieu M, Giraudet G, Betrouni N, Cosson M. 3D simulation of pelvic system numerical simulation for a better understanding of the contribution of the uterine ligaments. International urogynecology journal. 2013;24:2093–8. - PubMed
-
- Chanda A, Unnikrishnan V, Richter HE, Lockhart ME. A Biofidelic Computational Model of the Female Pelvic System to Understand Effect of Bladder Fill and Progressive Vaginal Tissue Stiffening due to Prolapse on Anterior Vaginal Wall. International journal for numerical methods in biomedical engineering. 2016 Jan 5; [Epub ahead of print] - PubMed
-
- Chen ZW, Joli P, Feng ZQ, Rahim M, Pirro N, Bellemare ME. Female patient-specific finite element modeling of pelvic organ prolapse (POP) Journal of biomechanics. 2015;48:238–45. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
