

Exploring the basic science of prolapse meshes
- PMID: 27517341
- PMCID: PMC5161092
- DOI: 10.1097/GCO.0000000000000313
Exploring the basic science of prolapse meshes
Abstract
Purpose of review: Polypropylene mesh has been widely used in the surgical repair of pelvic organ prolapse. However, low but persistent rates of complications related to mesh, most commonly mesh exposure and pain, have hampered its use. Complications are higher following transvaginal implantation prompting the Food and Drug Administration to release two public health notifications warning of complications associated with transvaginal mesh use (PHN 2008 and 2011) and to upclassify transvaginal prolapse meshes from Class II to Class III devices. Although there have been numerous studies to determine the incidence and management of mesh complications as well as impact on quality of life, few studies have focused on mechanisms.
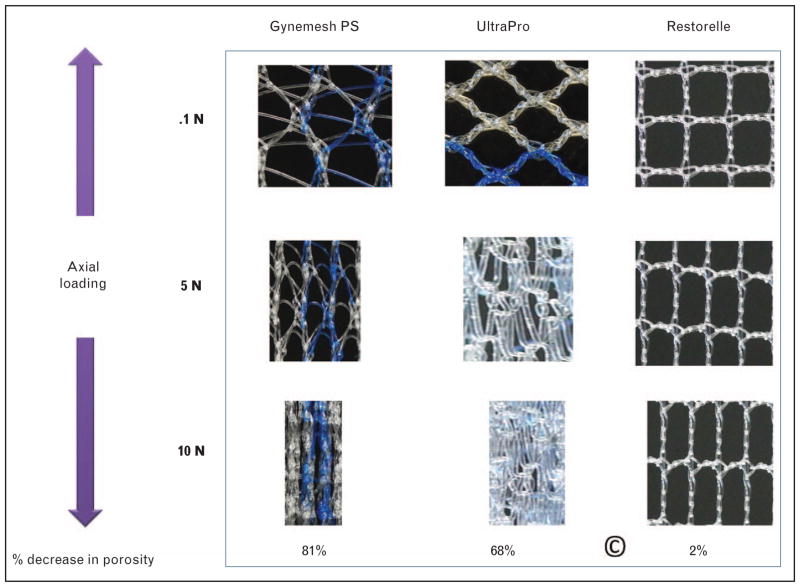
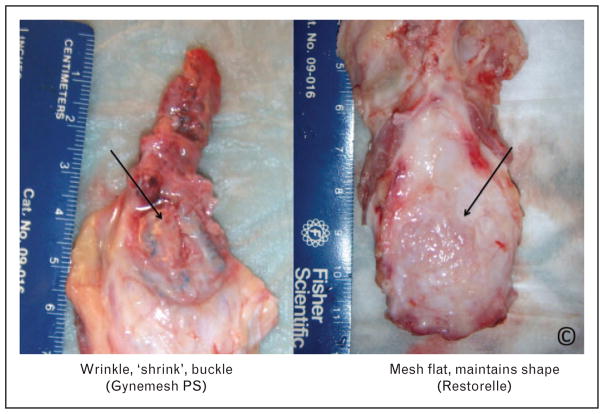
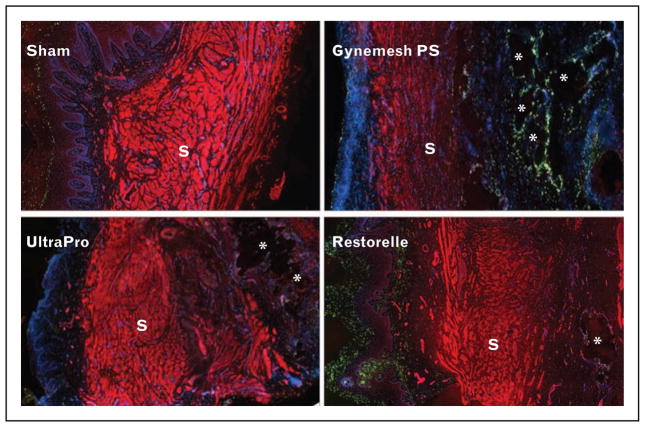
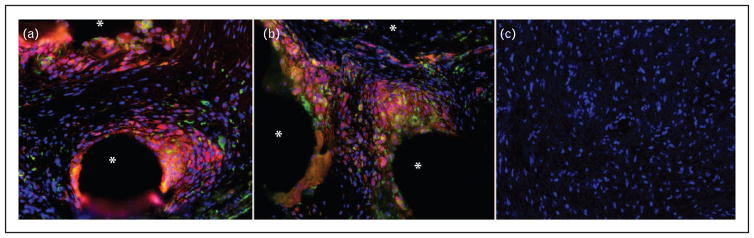
Recent findings: In this review, we summarize the current understanding of how mesh textile properties and mechanical behavior impact vaginal structure and function, as well as the local immune response. We also discuss how mesh properties change in response to loading.
Summary: We highlight a few areas of current and future research to emphasize collaborative strategies that incorporate basic science research to improve patient outcomes.
Conflict of interest statement
There are no conflicts of interest.
Figures
References
-
- Maher C, Baessler K. Surgical management of anterior vaginal wall prolapse: an evidence based literature review. Int Urogynecol J Pelvic Floor Dysfunct. 2006;17:195–201. - PubMed
-
- Mistrangelo E, Mancuso S, Nadalini C, et al. Rising use of synthetic mesh in transvaginal pelvic reconstructive surgery: a review of the risk of vaginal erosion. J Minim Invasive Gynecol. 2007;14:564–569. - PubMed
-
- Shah AD, Kohli N, Rajan SS, et al. The age distribution, rates, and types of surgery for pelvic organ prolapse in the USA. Int Urogynecol J Pelvic Floor Dysfunct. 2008;19:421–428. - PubMed
-
- Maher C, Feiner B, Baessler K, et al. Transvaginal mesh or grafts compared with native tissue repair for vaginal prolapse. Cochrane Database Syst Rev. 2016;2:CD012079. This is the most recent comprehensive review of randomized controlled trials comparing different types of vaginal repair (mesh, biological graft, or native tissue). This article suggests that the transvaginal mesh has limited utility in primary surgery based on the risk-benefit profile. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
