

Long-term outcome in ICU patients with acute kidney injury treated with renal replacement therapy: a prospective cohort study
- PMID: 27520553
- PMCID: PMC4983760
- DOI: 10.1186/s13054-016-1409-z
Long-term outcome in ICU patients with acute kidney injury treated with renal replacement therapy: a prospective cohort study
Abstract
Background: In intensive care unit (ICU) patients, acute kidney injury treated with renal replacement therapy (AKI-RRT) is associated with adverse outcomes. The aim of this study was to evaluate variables associated with long-term survival and kidney outcome and to assess the composite endpoint major adverse kidney events (MAKE; defined as death, incomplete kidney recovery, or development of end-stage renal disease treated with RRT) in a cohort of ICU patients with AKI-RRT.
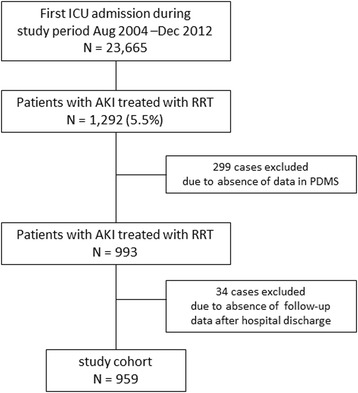
Methods: We conducted a single-center, prospective observational study in a 50-bed ICU tertiary care hospital. During the study period from August 2004 through December 2012, all consecutive adult patients with AKI-RRT were included. Data were prospectively recorded during the patients' hospital stay and were retrieved from the hospital databases. Data on long-term follow-up were gathered during follow-up consultation or, in the absence of this, by consulting the general physician.
Results: AKI-RRT was reported in 1292 of 23,665 first ICU admissions (5.5 %). Mortality increased from 59.7 % at hospital discharge to 72.1 % at 3 years. A Cox proportional hazards model demonstrated an association of increasing age, severity of illness, and continuous RRT with long-term mortality. Among hospital survivors with reference creatinine measurements, 1-year renal recovery was complete in 48.4 % and incomplete in 32.6 %. Dialysis dependence was reported in 19.0 % and was associated with age, diabetes, chronic kidney disease (CKD), and oliguria at the time of initiation of RRT. MAKE increased from 83.1 % at hospital discharge to 93.7 % at 3 years. Multivariate regression analysis showed no association of classical determinants of outcome (preexisting CKD, timing of initiation of RRT, and RRT modality) with MAKE at 1 year.
Conclusions: Our study demonstrates poor long-term survival after AKI-RRT that was determined mainly by severity of illness and RRT modality at initiation of RRT. Renal recovery is limited, especially in patients with acute-on-chronic kidney disease, making nephrological follow-up imperative. MAKE is associated mainly with variables determining mortality.
Keywords: Acute kidney injury (AKI); Acute-on-chronic kidney failure; Long-term survival; Major adverse kidney events (MAKE); Modality of renal replacement therapy; Renal recovery; Renal replacement therapy (RRT); Timing of renal replacement therapy.
Figures



References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
