

Gd-EOB-DTPA-enhanced magnetic resonance imaging combined with T1 mapping predicts the degree of differentiation in hepatocellular carcinoma
- PMID: 27520833
- PMCID: PMC4983030
- DOI: 10.1186/s12885-016-2607-4
Gd-EOB-DTPA-enhanced magnetic resonance imaging combined with T1 mapping predicts the degree of differentiation in hepatocellular carcinoma
Abstract
Background: Variable degrees of differentiation in hepatocellular carcinoma(HCC)under Edmondson-Steiner grading system has been proven to be an independent prognostic indicator for HCC. Up till now, there has been no effective radiological method that can reveal the degree of differentiation in HCC before surgery. This paper aims to evaluate the use of Gd-EOB-DTPA-Enhanced Magnetic Resonance Imaging combined with T1 mapping for the diagnosis of HCC and assessing its degree of differentiation.
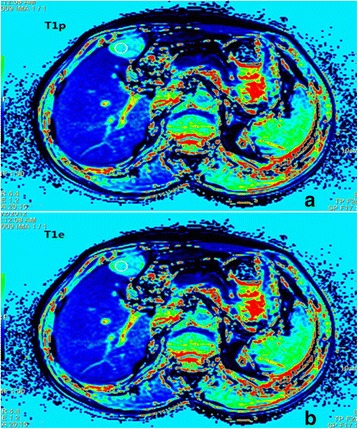
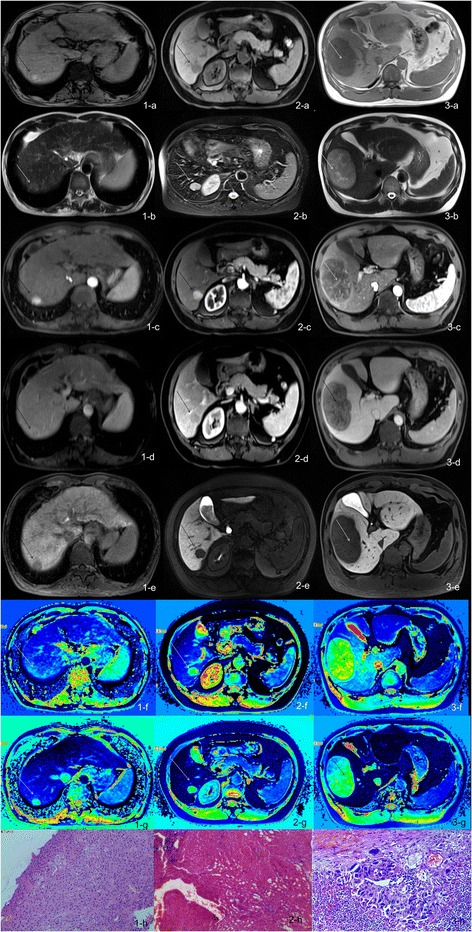
Methods: Forty-four patients with 53 pathologically proven HCC had undergone Gd-EOB-DTPA enhanced MRI with T1 mapping before surgery. Out of the 53 lesions,13 were grade I, 27 were gradeII, and 13 were grade III. The T1 values of each lesion were measured before and at 20 min after Gd-EOB-DTPA administration (T1p and T1e). The absolute reduction in T1 value (T1d) and the percentage reduction (T1d %) were calculated. The one-way ANOVA and Pearson correlation were used for comparisons between the T1 mapping values.
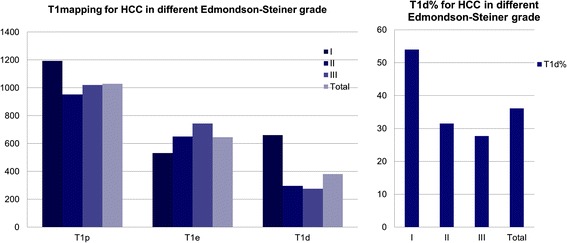
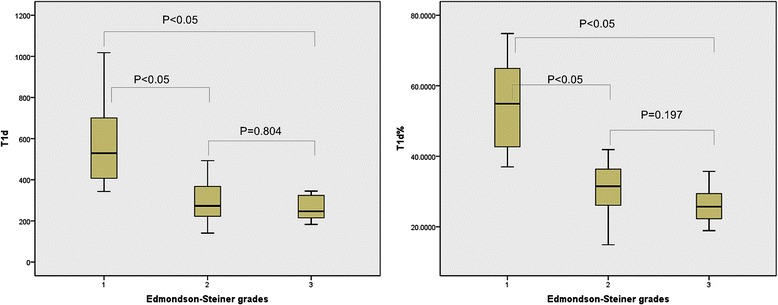
Results: The T1d and T1d % of grade I, II and III of HCC was 660.5 ± 422.8ms、295.0 ± 99.6ms、276.2 ± 95.0ms and 54.0 ± 12.2 %、31.5 ± 6.9 %、27.7 ± 6.7 % respectively. The differences between grade Iand II, grade Iand III were statistically significant (p < 0.05), but there was no statically significant difference between grade II and III. The T1d % was the best marker for grading of HCC, with a Spearman correlation coefficient of -0.676.
Conclusions: T1 mapping before and after Gd-EOB-DTPA administration can predict degree of differentiation in HCC.
Keywords: Differentiated degrees; Edmondson-Steiner grade; Gd-EOB-DTPA; Hepatocellular Carcinoma; T1 mapping.
Figures
Similar articles
-
T1 mapping combined with Gd-EOB-DTPA-enhanced magnetic resonance imaging in predicting the pathologic grading of hepatocellular carcinoma.J Biol Regul Homeost Agents. 2017 Oct-Dec;31(4):1029-1036. J Biol Regul Homeost Agents. 2017. PMID: 29254310
-
The Combination of Gd-EOB-DTPA Enhanced T1 Mapping with Apparent Diffusion Coefficient could Improve the Diagnostic Efficacy of Hepatocellular Carcinoma Grading.Curr Med Imaging. 2024;20:e15734056259418. doi: 10.2174/0115734056259418231112102249. Curr Med Imaging. 2024. PMID: 38918998
-
Evaluation of combined Gd-EOB-DTPA and gadobutrol magnetic resonance imaging for the prediction of hepatocellular carcinoma grading.Acta Radiol. 2016 Aug;57(8):932-8. doi: 10.1177/0284185115616293. Epub 2015 Nov 18. Acta Radiol. 2016. PMID: 26586852
-
Application of Gd-EOB-DTPA-enhanced magnetic resonance imaging (MRI) in hepatocellular carcinoma.World J Surg Oncol. 2020 Aug 22;18(1):219. doi: 10.1186/s12957-020-01996-4. World J Surg Oncol. 2020. PMID: 32828123 Free PMC article. Review.
-
Is Gadoxetic Acid Disodium (Gd-EOB-DTPA)-Enhanced Magnetic Resonance Imaging an Accurate Diagnostic Method for Hepatocellular Carcinoma? A Systematic Review with Meta-Analysis.Curr Med Imaging. 2022;18(6):633-647. doi: 10.2174/1573405617666210917124404. Curr Med Imaging. 2022. PMID: 34533447
Cited by
-
[Prediction of microvascular invasion in hepatocellular carcinoma with magnetic resonance imaging using models combining deep attention mechanism with clinical features].Nan Fang Yi Ke Da Xue Xue Bao. 2023 May 20;43(5):839-851. doi: 10.12122/j.issn.1673-4254.2023.05.21. Nan Fang Yi Ke Da Xue Xue Bao. 2023. PMID: 37313827 Free PMC article. Chinese.
-
Native T1 Mapping Magnetic Resonance Imaging as a Quantitative Biomarker for Characterization of the Extracellular Matrix in a Rabbit Hepatic Cancer Model.Biomedicines. 2020 Oct 13;8(10):412. doi: 10.3390/biomedicines8100412. Biomedicines. 2020. PMID: 33066169 Free PMC article.
-
T1 mapping-based radiomics in the identification of histological types of lung cancer: a reproducibility and feasibility study.BMC Med Imaging. 2024 Nov 14;24(1):308. doi: 10.1186/s12880-024-01487-y. BMC Med Imaging. 2024. PMID: 39543517 Free PMC article.
-
Diagnostic Value of Imaging Methods in the Histological Four Grading of Hepatocellular Carcinoma.Diagnostics (Basel). 2020 May 19;10(5):321. doi: 10.3390/diagnostics10050321. Diagnostics (Basel). 2020. PMID: 32438701 Free PMC article.
-
Advanced Imaging of Hepatocellular Carcinoma: A Review of Current and Novel Techniques.J Gastrointest Cancer. 2024 Dec;55(4):1469-1484. doi: 10.1007/s12029-024-01094-8. Epub 2024 Aug 19. J Gastrointest Cancer. 2024. PMID: 39158837 Review.
References
-
- Cancer research UK http://www.cancerresearchuk.org/health-professional/cancer-statistics/wo... 2014;2:14
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
