

A case of optic-nerve hypoplasia and anterior segment abnormality associated with facial cleft
- PMID: 27524922
- PMCID: PMC4965226
- DOI: 10.2147/IMCRJ.S99237
A case of optic-nerve hypoplasia and anterior segment abnormality associated with facial cleft
Abstract
Introduction: The incidence of facial cleft is rare and ranges between 1.43 and 4.85 per 100,000 births. To date, there have been few reports of detailed ophthalmologic examinations performed in cases of facial cleft. Here, we report a case of optic-nerve hypoplasia and anterior segment abnormality associated with facial cleft.
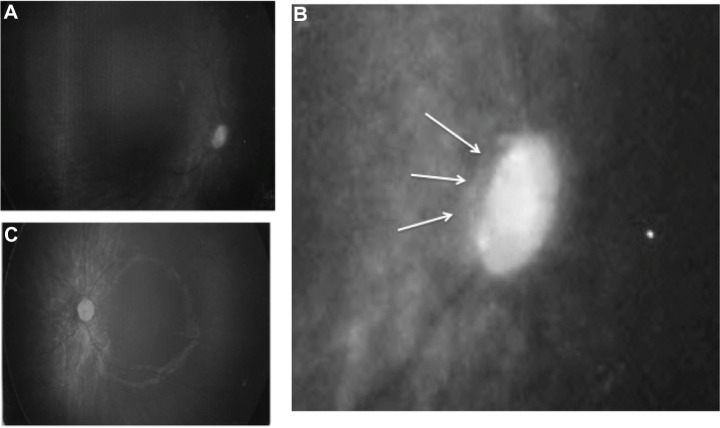
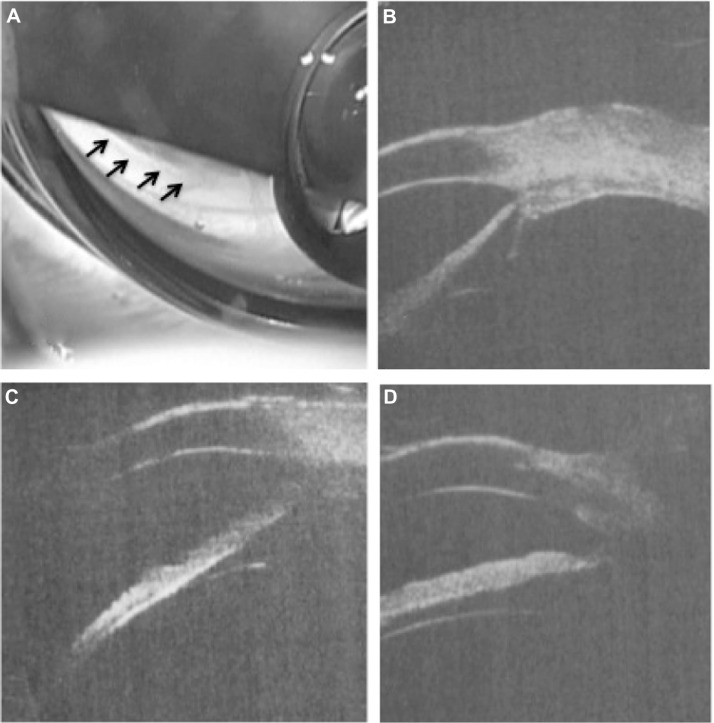
Case report: A 9-day-old female infant was delivered by cesarian section at 34 weeks of gestational age (the second baby of twins) and weighed 2,276 g upon presentation. She had a facial cleft and ectrodactyly at birth. Right eye-dominant blepharophimosis was obvious. Examination of the right eye revealed inferior corneal opacity with vascularization, downward corectopia, and optic-nerve hypoplasia. The corneal diameter was 8 mm in both eyes, and tonometry by use of a Tono-Pen(®) XL (Reichert Technologies, Depew, NY, USA) handheld applanation tonometer revealed that her intraocular pressure was 11-22 mmHg (Oculus Dexter) and 8 mmHg (Oculus Sinister). B-mode echo revealed no differences in axial length between her right and left eyes. When she was 15-16 months old, we attempted to examine her eyes before she underwent plastic surgery under general anesthesia. She had a small optic disc in both eyes and the right-eye disc was tilted. After undergoing canthotomy, gonioscopy and ultrasound biomicroscopy revealed that almost all directions were open except for the peripheral anterior synechia. Since magnetic resonance imaging revealed ventriculomegaly associated with an interhemispheric cyst at birth, a ventriculoperitoneal shunt was inserted at 12 days of age. At 25 months of age, her condition suddenly deteriorated due to occlusion of the ventricular shunt catheter, and she died 5 days later. In this patient, amniotic band syndrome was presumed to be the primary cause due to the clinical findings.
Conclusion: We experienced a case of optic-nerve hypoplasia and anterior segment abnormality that occurred with facial cleft. The cause of these abnormalities is unclear, yet amniotic band syndrome is a possible candidate.
Keywords: amniotic band syndrome; facial cleft; optic-nerve hypoplasia.
Figures



Similar articles
-
A rare case of cleft number nine associated with atypical cleft number two.Indian J Ophthalmol. 2017 Jul;65(7):610-612. doi: 10.4103/ijo.IJO_914_16. Indian J Ophthalmol. 2017. PMID: 28724820 Free PMC article.
-
Comparison of two handheld applanation tonometers and the association of central corneal thickness, age, and intraocular pressure in normal and diseased canine eyes.Vet Ophthalmol. 2014 Nov;17(6):417-25. doi: 10.1111/vop.12151. Epub 2014 Feb 12. Vet Ophthalmol. 2014. PMID: 24517734
-
[Optic Disc Drusen and their Complications].Cesk Slov Oftalmol. 2016 Feb;72(1):298-308. Cesk Slov Oftalmol. 2016. PMID: 27041286 Czech.
-
Blindness as a complication of Le Fort I osteotomy for maxillary distraction.Plast Reconstr Surg. 2002 Feb;109(2):688-98; discussion 699-700. doi: 10.1097/00006534-200202000-00041. Plast Reconstr Surg. 2002. PMID: 11818854 Review.
-
Rathke's cleft cyst presenting as incomplete cavernous sinus syndrome and disc edema: a case report with literature review.Doc Ophthalmol. 2020 Feb;140(1):55-65. doi: 10.1007/s10633-019-09713-7. Epub 2019 Sep 6. Doc Ophthalmol. 2020. PMID: 31493011 Review.
Cited by
-
Whole genome sequencing reveals translocation breakpoints disrupting TP63 gene underlying split hand/foot malformation in a Chinese family.Mol Genet Genomic Med. 2021 Mar;9(3):e1604. doi: 10.1002/mgg3.1604. Epub 2021 Jan 20. Mol Genet Genomic Med. 2021. PMID: 33471964 Free PMC article.
References
-
- Kawamoto HK., Jr The kaleidoscopic world of rare craniofacial clefts: order out of chaos (Tessier classification) Clin Plast Surg. 1976;3(4):529–572. - PubMed
-
- Tessier P. Anatomical classification of facial, cranio-facial and latero-facial clefts. J Maxillofac Surg. 1976;4(2):69–92. - PubMed
-
- Coruh A, Gunay GK. A surgical conundrum: Tessier number 4 cleft. Cleft Palate Craniofac J. 2005;42(1):102–106. - PubMed
-
- David DJ, Moore MH, Cooter RD. Tessier clefts revisited with a third dimension. Cleft Palate J. 1989;26(3):163–185. - PubMed
-
- Whitaker LA, Katowitz JA, Randall P. The nasolacrimal apparatus in congenital facial anomalies. J Maxillofac Surg. 1974;2(2–3):59–63. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
