

How Do Antihypertensive Drugs Work? Insights from Studies of the Renal Regulation of Arterial Blood Pressure
- PMID: 27524972
- PMCID: PMC4965470
- DOI: 10.3389/fphys.2016.00320
How Do Antihypertensive Drugs Work? Insights from Studies of the Renal Regulation of Arterial Blood Pressure
Abstract
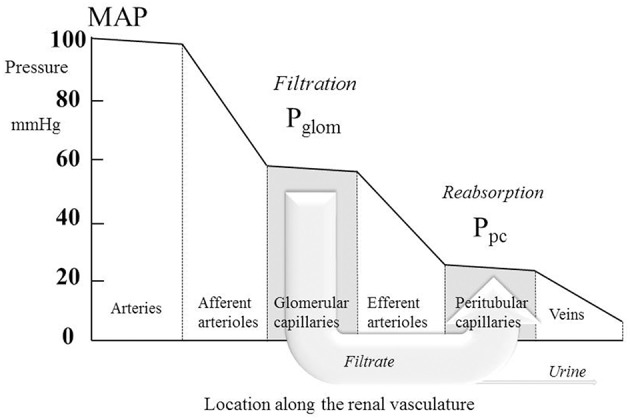
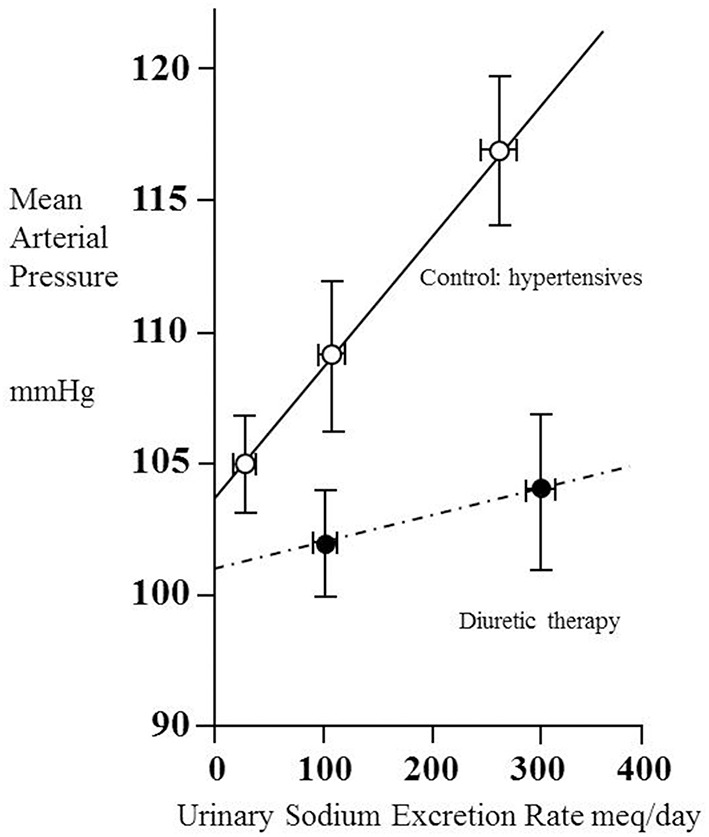
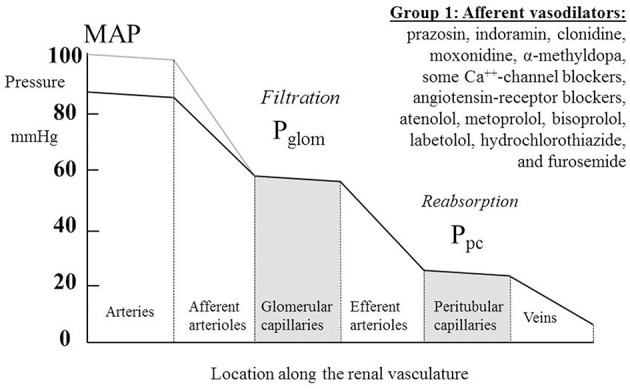
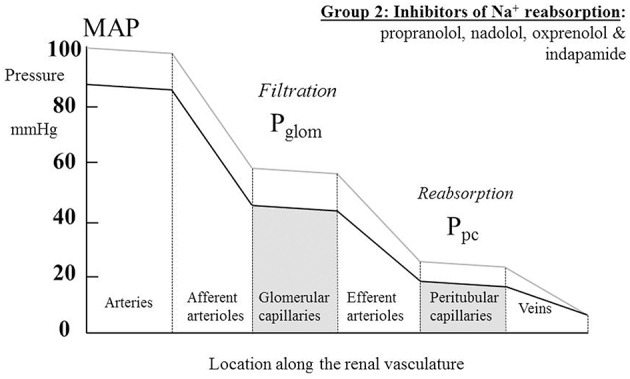
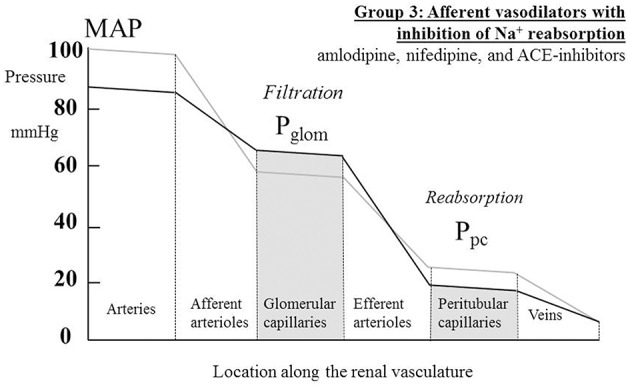
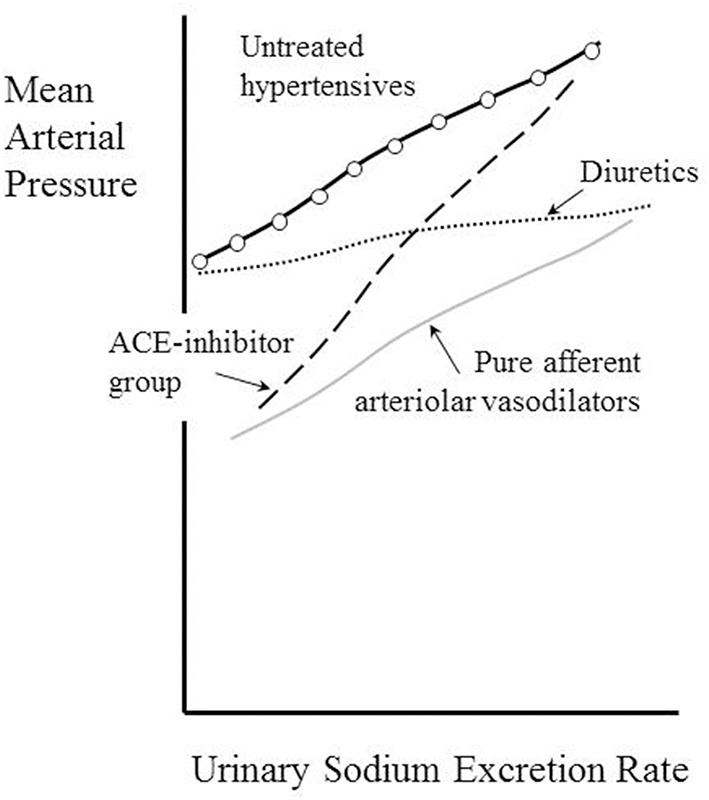
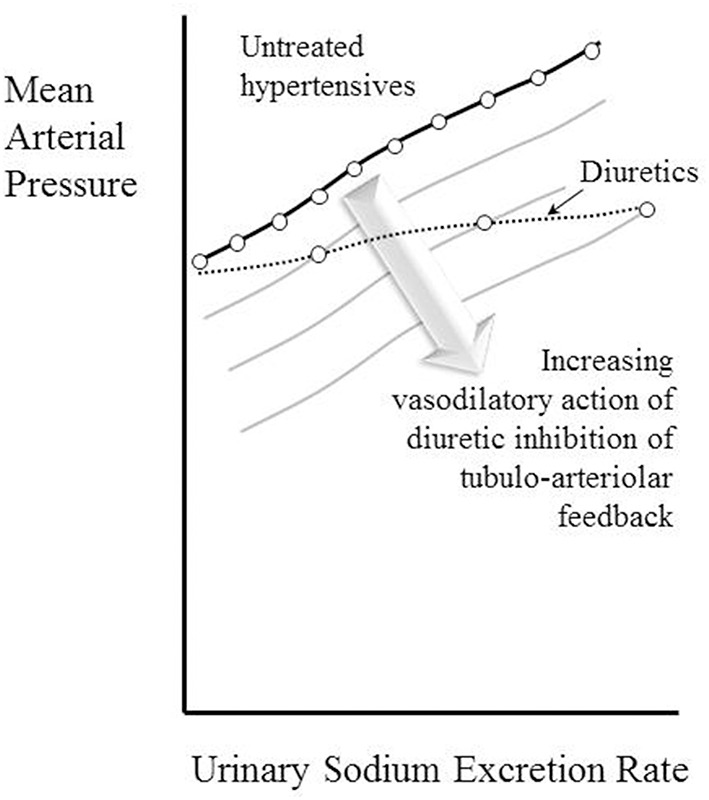
Though antihypertensive drugs have been in use for many decades, the mechanisms by which they act chronically to reduce blood pressure remain unclear. Over long periods, mean arterial blood pressure must match the perfusion pressure necessary for the kidney to achieve its role in eliminating the daily intake of salt and water. It follows that the kidney is the most likely target for the action of most effective antihypertensive agents used chronically in clinical practice today. Here we review the long-term renal actions of antihypertensive agents in human studies and find three different mechanisms of action for the drugs investigated. (i) Selective vasodilatation of the renal afferent arteriole (prazosin, indoramin, clonidine, moxonidine, α-methyldopa, some Ca(++)-channel blockers, angiotensin-receptor blockers, atenolol, metoprolol, bisoprolol, labetolol, hydrochlorothiazide, and furosemide). (ii) Inhibition of tubular solute reabsorption (propranolol, nadolol, oxprenolol, and indapamide). (iii) A combination of these first two mechanisms (amlodipine, nifedipine and ACE-inhibitors). These findings provide insights into the actions of antihypertensive drugs, and challenge misconceptions about the mechanisms underlying the therapeutic efficacy of many of the agents.
Keywords: antihypertensive drugs; diuretics; hypertension; renal circulation; vasodilator agents.
Figures
Similar articles
-
THE NITROSAMINE CONTAMINATION IN BETA BLOCKERS (BISOPROLOL/METOPROLOL), ACE INHIBITORS (LISINOPRIL/PERINDOPRIL), THIAZIDES DIURETICS (HCT), CALCIUM CHANNEL BLOCKERS (AMLODIPINE/FELODIPINE), SARTANS (CANDESARTAN) AND ТHE SUBSEQUENT SKIN CANCER DEVELOPMENT AND PROGRESSION: APOCALYPSE NOW.Georgian Med News. 2023 Apr;(337):138-145. Georgian Med News. 2023. PMID: 37354687
-
[Are all antihypertensive drugs renoprotective?].Herz. 2004 May;29(3):248-54. doi: 10.1007/s00059-003-2508-6. Herz. 2004. PMID: 15167950 Review. German.
-
Drugs for hypertension.Med Lett Drugs Ther. 2020 May 18;62(1598):73-80. Med Lett Drugs Ther. 2020. PMID: 32555118 No abstract available.
-
Antihypertensive drug prescription trends at the primary health care centres in Bahrain.Pharmacoepidemiol Drug Saf. 2001 May;10(3):219-27. doi: 10.1002/pds.578. Pharmacoepidemiol Drug Saf. 2001. PMID: 11501335
-
Drugs for hypertension.Med Lett Drugs Ther. 2024 May 27;66(1703):81-88. doi: 10.58347/tml.2024.1703a. Med Lett Drugs Ther. 2024. PMID: 38771738 Review. No abstract available.
Cited by
-
Single-Cell Transcriptome Profiling of the Kidney Glomerulus Identifies Key Cell Types and Reactions to Injury.J Am Soc Nephrol. 2020 Oct;31(10):2341-2354. doi: 10.1681/ASN.2020020220. Epub 2020 Jul 10. J Am Soc Nephrol. 2020. PMID: 32651223 Free PMC article.
-
Mathematical modeling of antihypertensive therapy.Front Physiol. 2022 Dec 14;13:1070115. doi: 10.3389/fphys.2022.1070115. eCollection 2022. Front Physiol. 2022. PMID: 36589434 Free PMC article.
-
Effective prevention of sorafenib-related vascular damage induced adverse events and maintenance of hepatic function by dried bonito broth and histidine.Cancer Manag Res. 2019 May 13;11:4437-4448. doi: 10.2147/CMAR.S201424. eCollection 2019. Cancer Manag Res. 2019. PMID: 31191006 Free PMC article.
-
The Neurochemical Effects of Prazosin Treatment on Fear Circuitry in a Rat Traumatic Stress Model.Clin Psychopharmacol Neurosci. 2020 May 31;18(2):219-230. doi: 10.9758/cpn.2020.18.2.219. Clin Psychopharmacol Neurosci. 2020. PMID: 32329303 Free PMC article.
-
Dynamic tissue perfusion assessment reflects associations between antihypertensive treatment and renal cortical perfusion in patients with chronic kidney disease and hypertension.Int Urol Nephrol. 2018 Mar;50(3):509-516. doi: 10.1007/s11255-018-1798-9. Epub 2018 Jan 27. Int Urol Nephrol. 2018. PMID: 29374813 Free PMC article.
References
-
- Anderton J. L., Gill M., Notghi A. (1994). Renal haemodynamic effects of bunazosin retard and prazosin in mild to moderately hypertensive patients with normal or moderately impaired renal function. Nephrol. Dial. Trans. 9, 607–612. - PubMed
-
- Bauer J. H. (1984). Role of angiotensin converting enzyme inhibitors in essential and renal hypertension. Effects of captopril and enalapril on renin-angiotensin-aldosterone, renal function and hemodynamics, salt and water excretion, and body fluid composition. Am. J. Med. 77, 43–51. 10.1016/S0002-9343(84)80057-1 - DOI - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous