

Cerebral Blood Flow, Heart Rate, and Blood Pressure Patterns during the Tilt Test in Common Orthostatic Syndromes
- PMID: 27525257
- PMCID: PMC4972931
- DOI: 10.1155/2016/6127340
Cerebral Blood Flow, Heart Rate, and Blood Pressure Patterns during the Tilt Test in Common Orthostatic Syndromes
Abstract
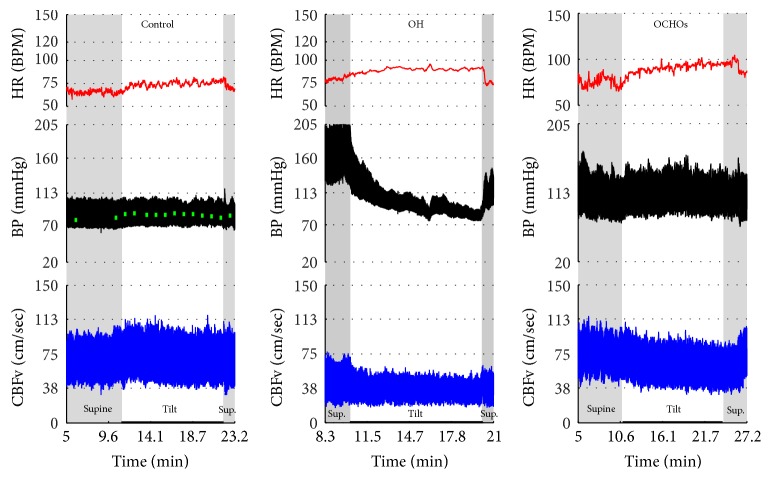
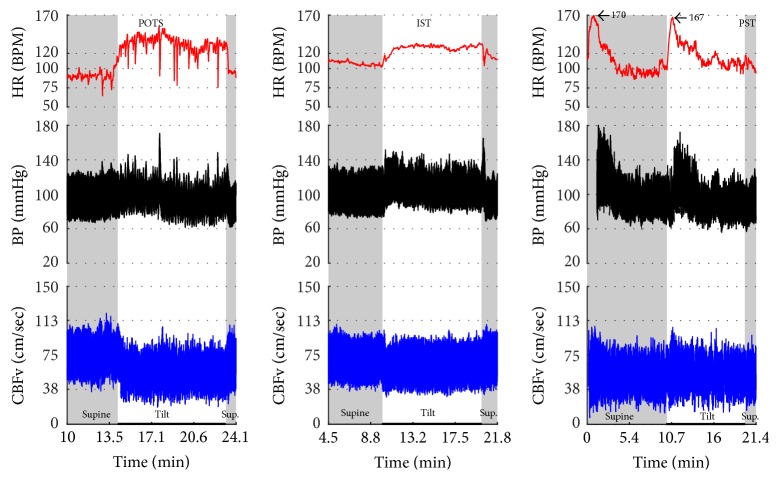
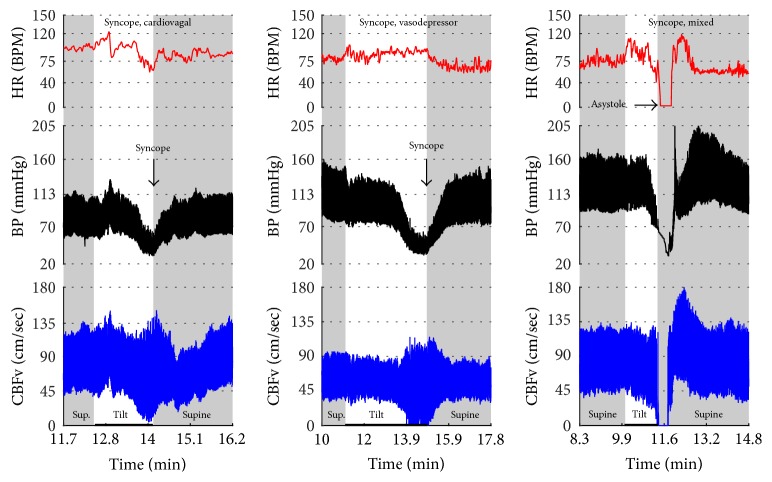
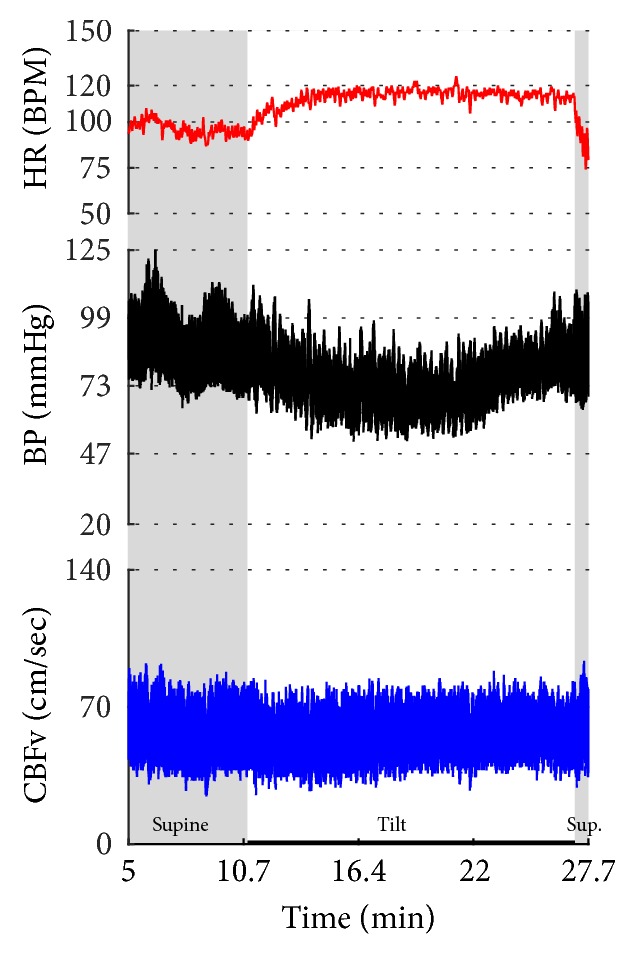
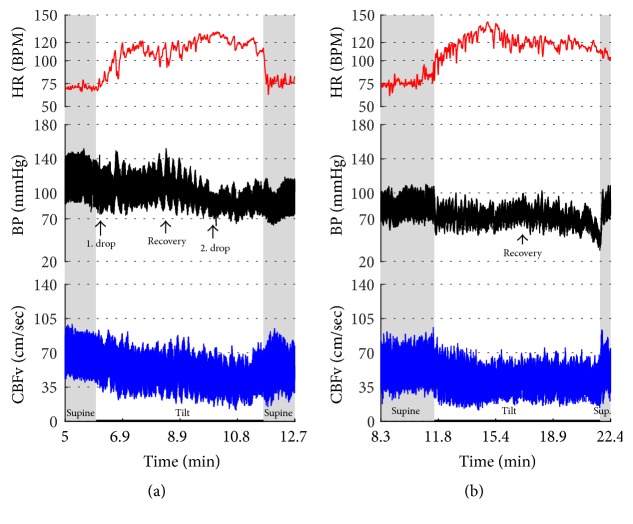
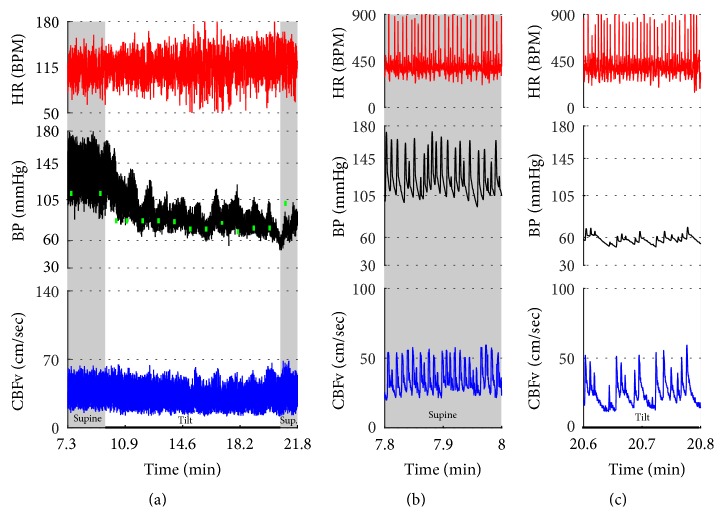
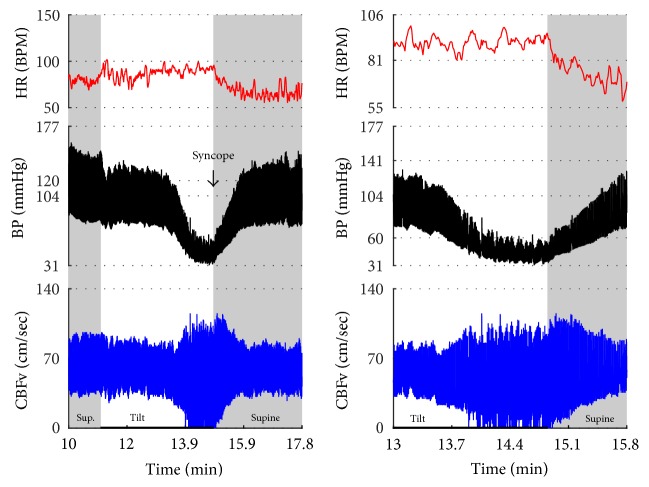
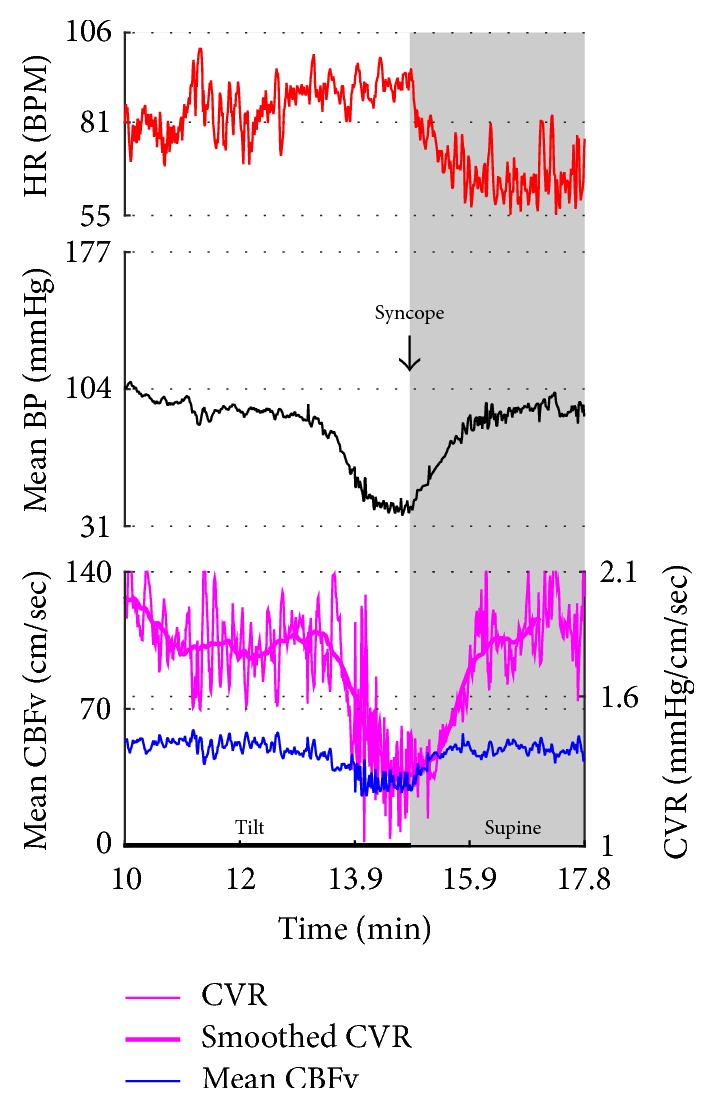
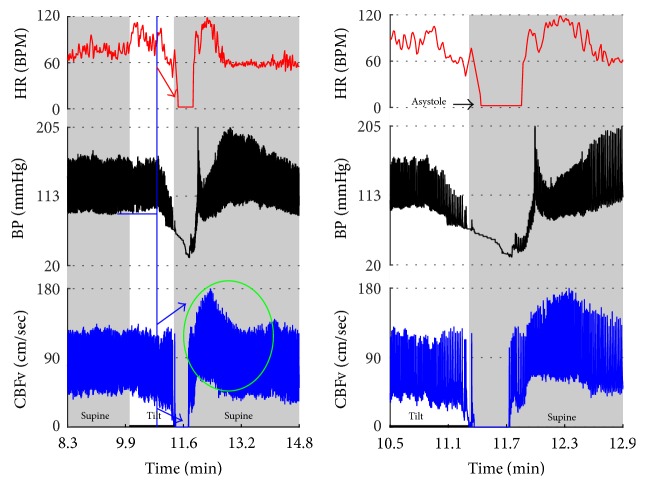
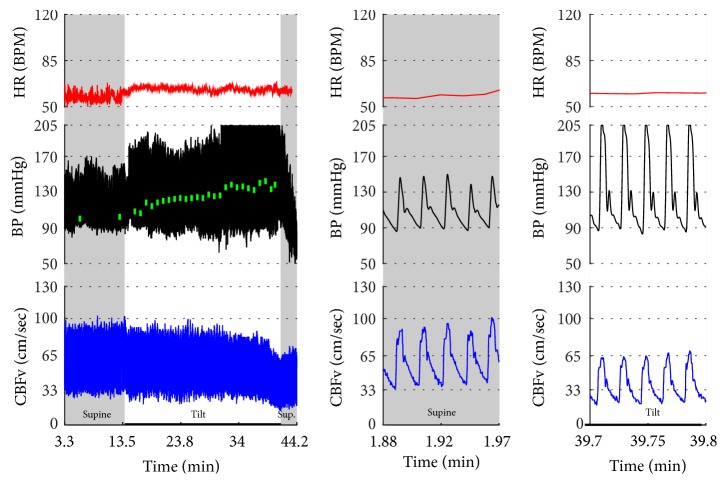
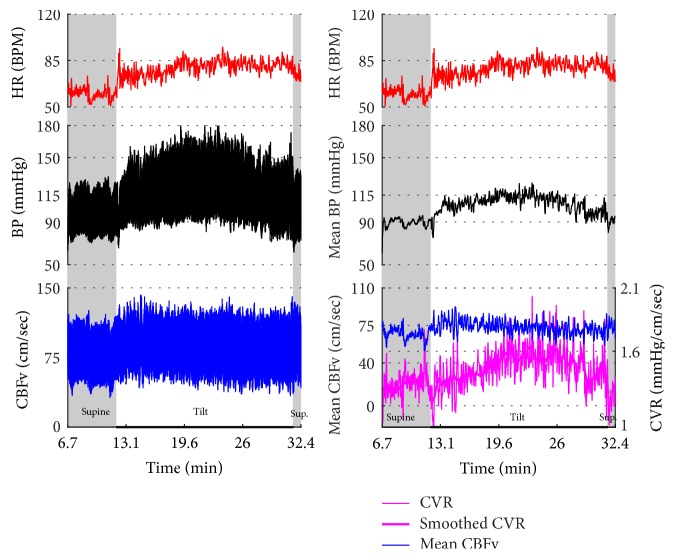
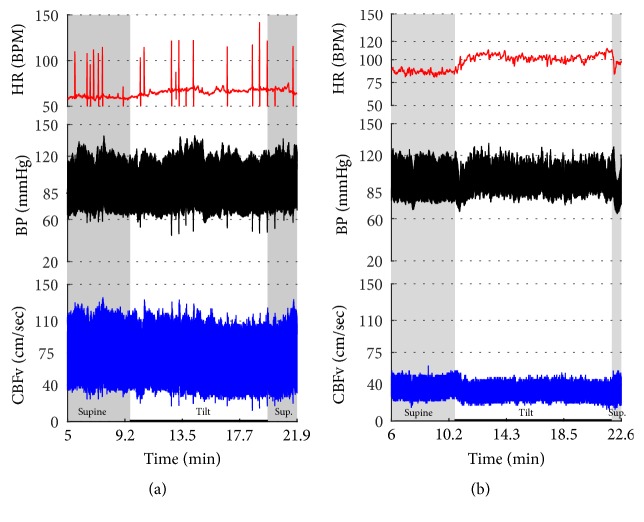
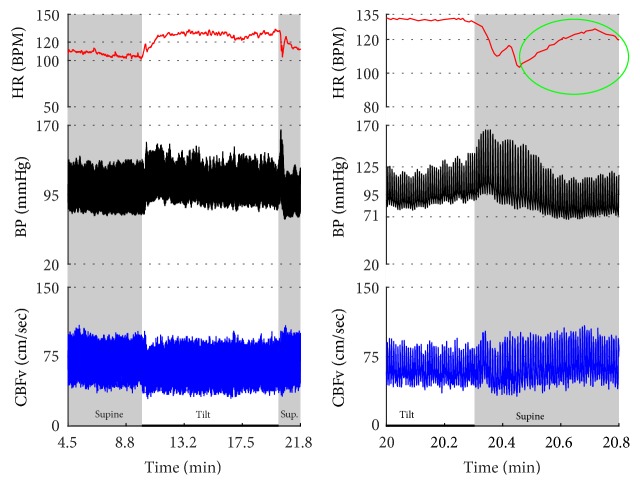
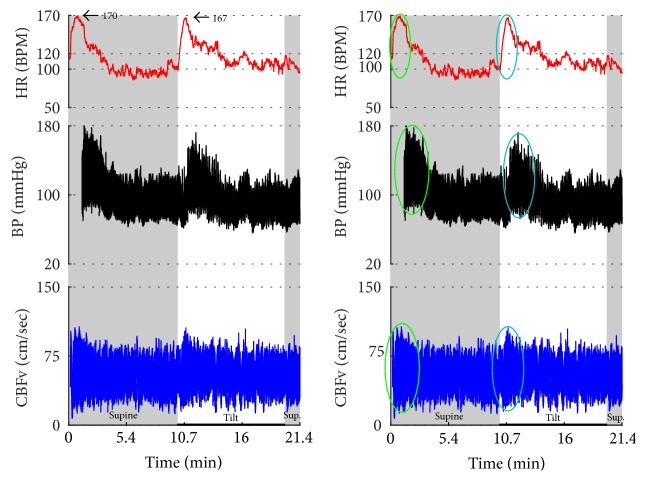
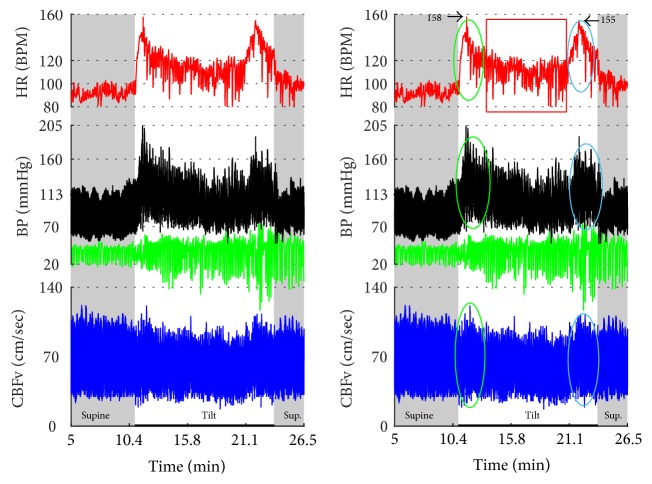
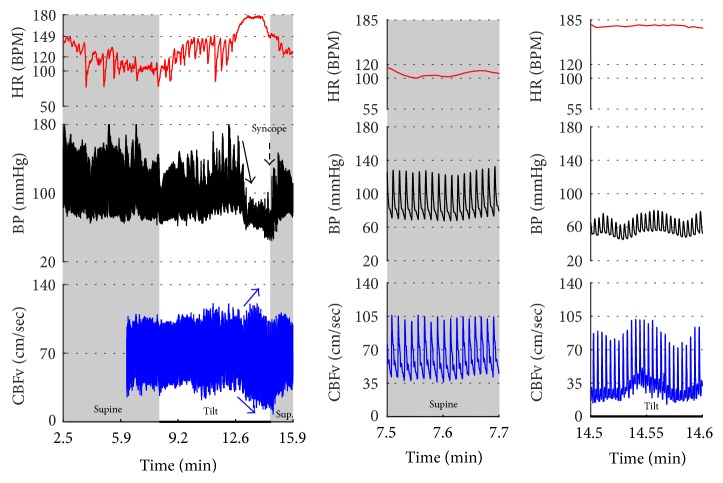
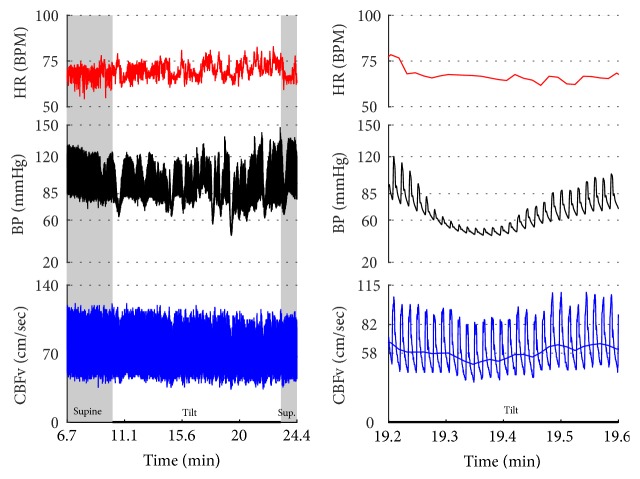
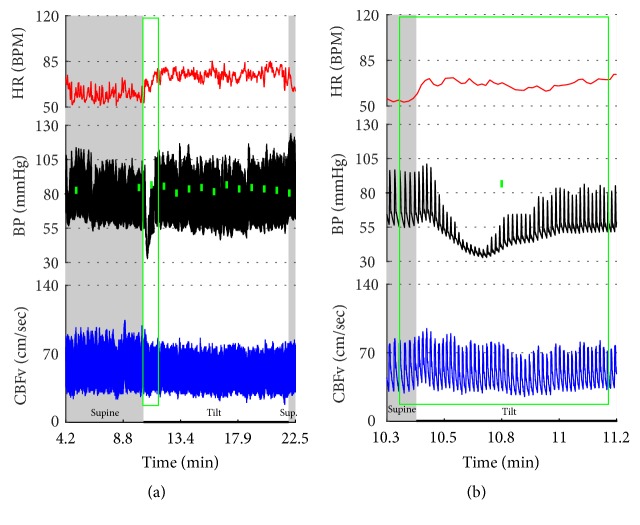
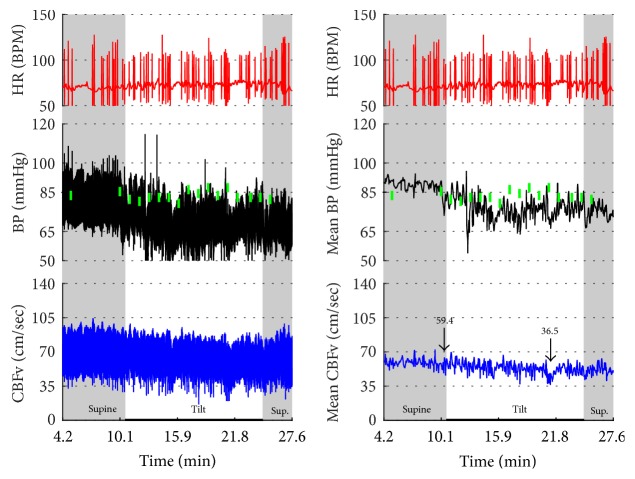
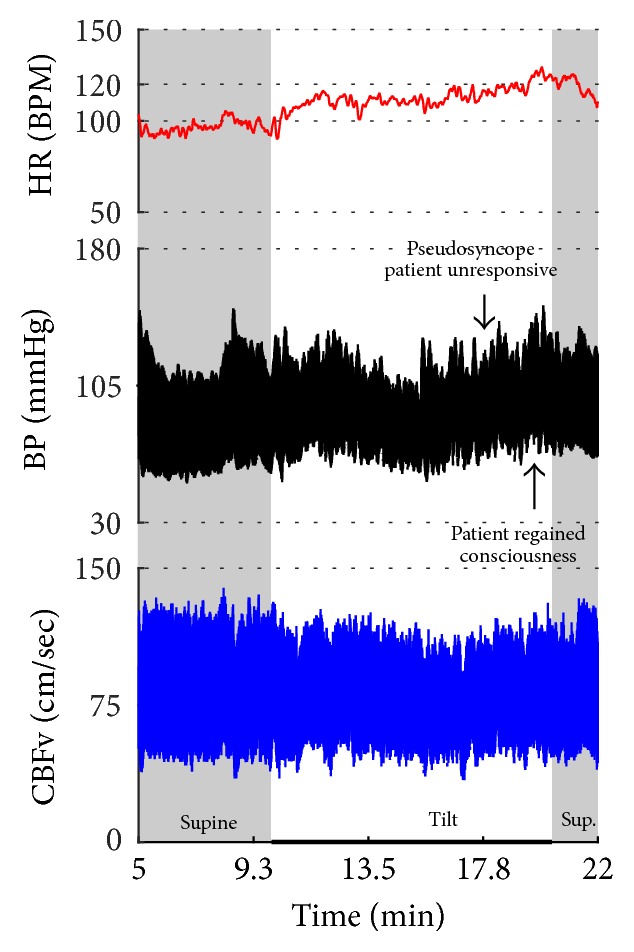
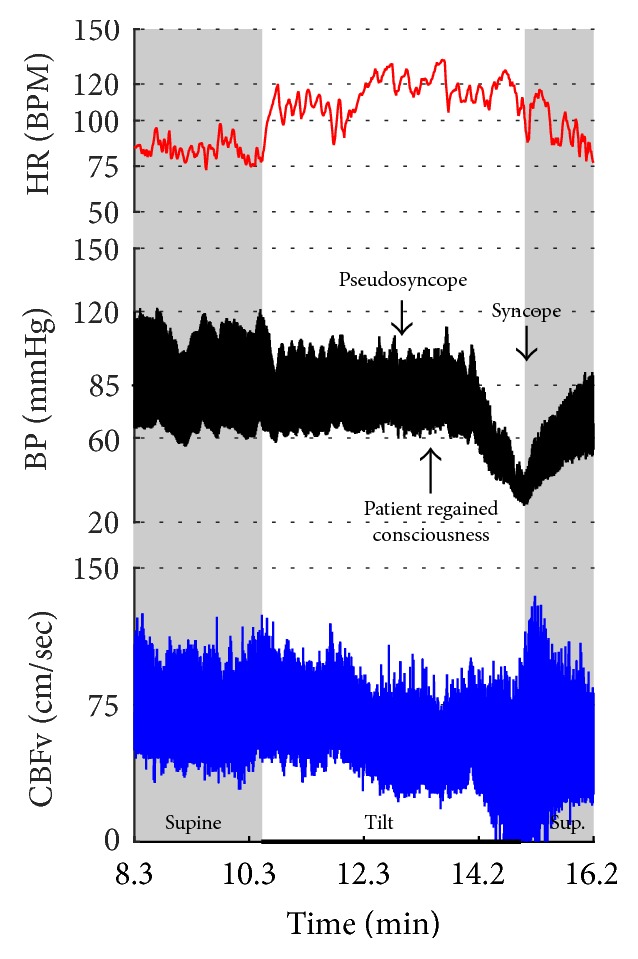
Objective. The head-up tilt test is widely used for evaluation of orthostatic intolerance. Although orthostatic symptoms usually reflect cerebral hypoperfusion, the cerebral blood flow velocity (CBFv) profile in orthostatic syndromes is not well described. This study evaluated CBFv and cardiovascular patterns associated with the tilt test in common orthostatic syndromes. Methods. This retrospective study analyzed the tilt test of patients with history of orthostatic intolerance. The following signals were recorded: ECG, blood pressure, CBFv using transcranial Doppler, respiratory signals, and end tidal CO2. Results. Data from 744 patients were analyzed. Characteristic pattern associated with a particular orthostatic syndrome can be grouped into abnormalities predominantly affecting blood pressure (orthostatic hypotension, orthostatic hypertension syndrome, vasomotor oscillations, and neurally mediated syncope-cardioinhibitory, vasodepressor, and mixed), cerebral blood flow (orthostatic hypoperfusion syndrome, primary cerebral autoregulatory failure), and heart rate (tachycardia syndromes: postural tachycardia syndrome, paroxysmal sinus tachycardia, and inappropriate sinus tachycardia). Psychogenic pseudosyncope is associated with stable CBFv. Conclusions. The tilt test is useful add-on in diagnosis of several orthostatic syndromes. However diagnostic criteria for several syndromes had to be modified to allow unambiguous pattern classification. CBFv monitoring in addition to blood pressure and heart rate may increase diagnostic yield of the tilt test.
Figures


References
-
- Kenny R. A., Ingram A., Bayliss J., Sutton R. Head-up tilt: a useful test for investigating unexplained syncope. The Lancet. 1986;1(8494):1352–1355. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
