

Physiotherapy scoliosis-specific exercises - a comprehensive review of seven major schools
- PMID: 27525315
- PMCID: PMC4973373
- DOI: 10.1186/s13013-016-0076-9
Physiotherapy scoliosis-specific exercises - a comprehensive review of seven major schools
Abstract
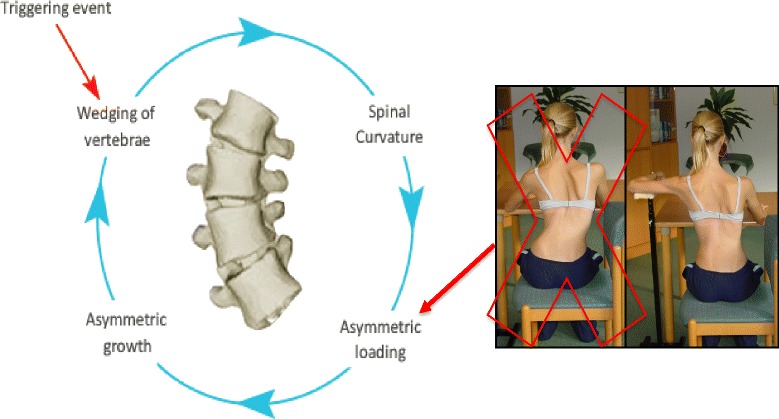
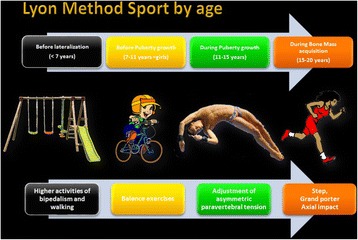
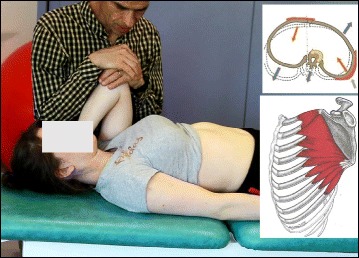
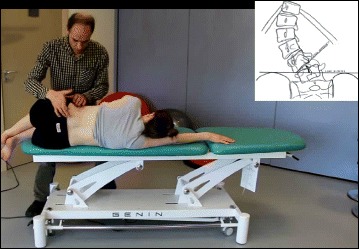
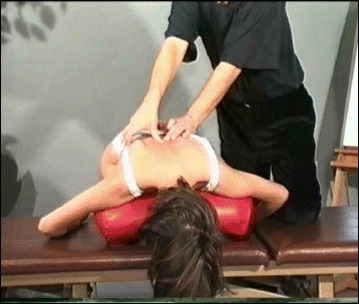
In recent decades, there has been a call for change among all stakeholders involved in scoliosis management. Parents of children with scoliosis have complained about the so-called "wait and see" approach that far too many doctors use when evaluating children's scoliosis curves between 10° and 25°. Observation, Physiotherapy Scoliosis Specific Exercises (PSSE) and bracing for idiopathic scoliosis during growth are all therapeutic interventions accepted by the 2011 International Society on Scoliosis Orthopaedic and Rehabilitation Treatment (SOSORT). The standard features of these interventions are: 1) 3-dimension self-correction; 2) Training activities of daily living (ADL); and 3) Stabilization of the corrected posture. PSSE is part of a scoliosis care model that includes scoliosis specific education, scoliosis specific physical therapy exercises, observation or surveillance, psychological support and intervention, bracing and surgery. The model is oriented to the patient. Diagnosis and patient evaluation is essential in this model looking at a patient-oriented decision according to clinical experience, scientific evidence and patient's preference. Thus, specific exercises are not considered as an alternative to bracing or surgery but as a therapeutic intervention, which can be used alone or in combination with bracing or surgery according to individual indication. In the PSSE model it is recommended that the physical therapist work as part of a multidisciplinary team including the orthopeadic doctor, the orthotist, and the mental health care provider - all are according to the SOSORT guidelines and Scoliosis Research Society (SRS) philosophy. From clinical experiences, PSSE can temporarily stabilize progressive scoliosis curves during the secondary period of progression, more than a year after passing the peak of growth. In non-progressive scoliosis, the regular practice of PSSE could produce a temporary and significant reduction of the Cobb angle. PSSE can also produce benefits in subjects with scoliosis other than reducing the Cobb angle, like improving back asymmetry, based on 3D self-correction and stabilization of a stable 3D corrected posture, as well as the secondary muscle imbalance and related pain. In more severe cases of thoracic scoliosis, it can also improve breathing function. This paper will discuss in detail seven major scoliosis schools and their approaches to PSSE, including their bracing techniques and scientific evidence. The aim of this paper is to understand and learn about the different international treatment methods so that physical therapists can incorporate the best from each into their own practices, and in that way attempt to improve the conservative management of patients with idiopathic scoliosis. These schools are presented in the historical order in which they were developed. They include the Lyon approach from France, the Katharina Schroth Asklepios approach from Germany, the Scientific Exercise Approach to Scoliosis (SEAS) from Italy, the Barcelona Scoliosis Physical Therapy School approach (BSPTS) from Spain, the Dobomed approach from Poland, the Side Shift approach from the United Kingdom, and the Functional Individual Therapy of Scoliosis approach (FITS) from Poland.
Figures





























References
-
- Schreiber S, Parent EC, Hedden DM, Hill D, Moreau MJ, Lou E, Watkins EM, Southon SC. The effect of Schroth exercises added to the standard of care on the quality of life and muscle endurance in adolescents with idiopathic scoliosis—an assessor and statistician blinded randomized controlled trial: “SOSORT 2015 Award Winner”. Scoliosis. 2015;10:24. doi: 10.1186/s13013-015-0048-5. - DOI - PMC - PubMed
-
- Weiss H, Moramarco M, Moramarco K. Risks and long-term complications of adolescent idiopathic scoliosis surgery vs. non-operative and natural history outcomes. Hard Tissue. 2013;2(3):27. doi: 10.13172/2050-2303-2-3-498. - DOI
-
- Negrini S, Hresko TM, O’Brien JP, Price N, SOSORT Boards and SRS Non-Operative Committee SOSORT Boards and SRS Non-Operative Committee Recommendations for research studies on treatment of idiopathic scoliosis: Consensus 2014 between SOSORT and SRS non–operative management committee. Scoliosis. 2015;10:8. doi: 10.1186/s13013-014-0025-4. - DOI - PMC - PubMed
-
- Monticone M, Ambrosini E, Cazzaniga D, Rocca B, ferrante S. Active self-correction and task-orientated exercises reduce spinal deformity and improve quality of life in subjects with mild adolescent idiopathic scoliosis. Results of a randomized controlled trial. Eur Spine J. 2014;23(6):1204–14. doi: 10.1007/s00586-014-3241-y. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous