

Sentinel lymph node detection rates using indocyanine green in women with early-stage cervical cancer
- PMID: 27526991
- PMCID: PMC5576021
- DOI: 10.1016/j.ygyno.2016.08.236
Sentinel lymph node detection rates using indocyanine green in women with early-stage cervical cancer
Abstract
Objective: Our study objective was to determine feasibility and mapping rates using indocyanine green (ICG) for sentinel lymph node (SLN) mapping in early-stage cervical cancer.
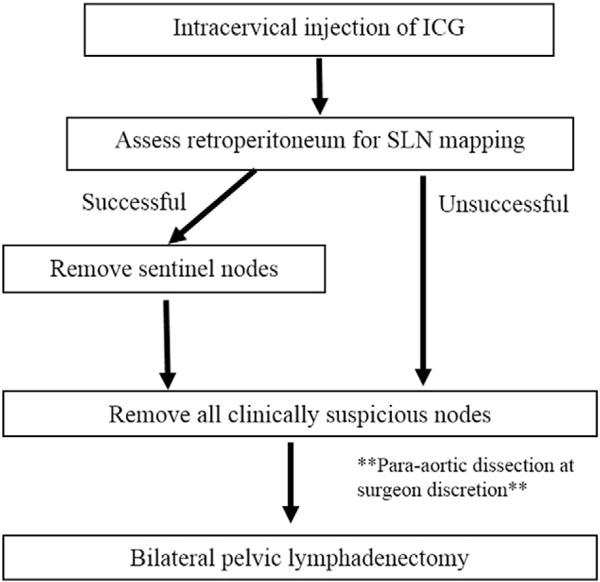
Methods: We performed a retrospective review of all women who underwent SLN mapping with ICG during primary surgical management of early-stage cervical cancer by robotic-assisted radical hysterectomy (RA-RH) or fertility-sparing surgery. Patients were treated at two high-volume centers from 10/2012 to 02/2016. Completion pelvic lymphadenectomy was performed after SLN biopsy; additionally, removal of clinically enlarged/suspicious nodes was part of the SLN treatment algorithm.
Results: Thirty women with a median age of 42.5 and BMI of 26.5 were included. Most (90%) had stage IB disease, and 67% had squamous histology. RA-RH was performed in 86.7% of cases. One patient underwent fertility-sparing surgery. Median cervical tumor size was 2.0cm. At least one SLN was detected in all cases (100%), with bilateral mapping achieved in 87%. SLN detection was not impacted by tumor size and was most commonly identified in the hypogastric (40.3%), obturator (26.0%), and external iliac (20.8%) regions. Five cases of lymphatic metastasis were identified (16.7%): three in clinically enlarged SLNs, one in a clinically enlarged non-SLN, and one case with cytokeratin positive cells in an SLN. All metastatic disease would have been detected even if full lymphadenectomy had been omitted from our treatment algorithm, CONCLUSIONS: SLN mapping with ICG is feasible and results in high detection rates in women with early-stage cervical cancer. Prospective studies are needed to determine if SLN mapping can replace lymphadenectomy in this setting.
Keywords: Cervical cancer; Fluorescence imaging; Indocyanine green; Robotic hysterectomy; Sentinel lymph node.
Copyright © 2016 Elsevier Inc. All rights reserved.
Conflict of interest statement
All authors confirm they have no conflict of interest to disclose.
Figures
References
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2015. CA Cancer J Clin. 2015;65:5–29. http://dx.doi.org/10.3322/caac.21254. - DOI - PubMed
-
- Howlader N FE, Noone AM, Krapcho M, Garshell J, Neyman N, Altekruse SF, Kosary CL, Yu M, Ruhl J, Tatalovich Z, Cho H, Mariotto A, Lewis DR, Chen HS. SEER Cancer Statistics Review, 1975–2010. National Cancer Institute; Bethesda, MD: http://seer.cancer.gov/csr/1975_2010/, based on November 2012 SEER data submission, posted to the SEER web site, April 2013., n.d.
-
- Fuller AF, Elliott N, Kosloff C, Hoskins WJ, Lewis JL. Determinants of increased risk for recurrence in patients undergoing radical hysterectomy for stage IB and IIA carcinoma of the cervix. Gynecol Oncol. 1989;33:34–39. http://www.ncbi.nlm.nih.gov/pubmed/2703164 (accessed February 10, 2016) - PubMed
-
- Kato T, Watari H, Takeda M, Hosaka M, Mitamura T, Kobayashi N, et al. Multivariate prognostic analysis of adenocarcinoma of the uterine cervix treated with radical hysterectomy and systematic lymphadenectomy. J Gynecol Oncol. 2013;24:222–228. http://dx.doi.org/10.3802/jgo.2013.24.3.222. - DOI - PMC - PubMed
-
- Havrilesky LJ, Leath CA, Huh W, Calingaert B, Bentley RC, Soper JT, et al. Radical hysterectomy and pelvic lymphadenectomy for stage IB2 cervical cancer. Gynecol Oncol. 2004;93:429–434. http://dx.doi.org/10.1016/j.ygyno.2004.01.038. - DOI - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
