

Urinary π-glutathione S-transferase Predicts Advanced Acute Kidney Injury Following Cardiovascular Surgery
- PMID: 27527370
- PMCID: PMC4985825
- DOI: 10.1038/srep26335
Urinary π-glutathione S-transferase Predicts Advanced Acute Kidney Injury Following Cardiovascular Surgery
Abstract
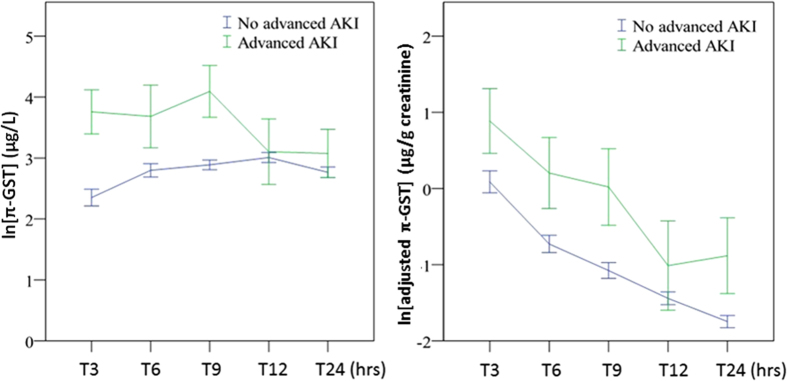
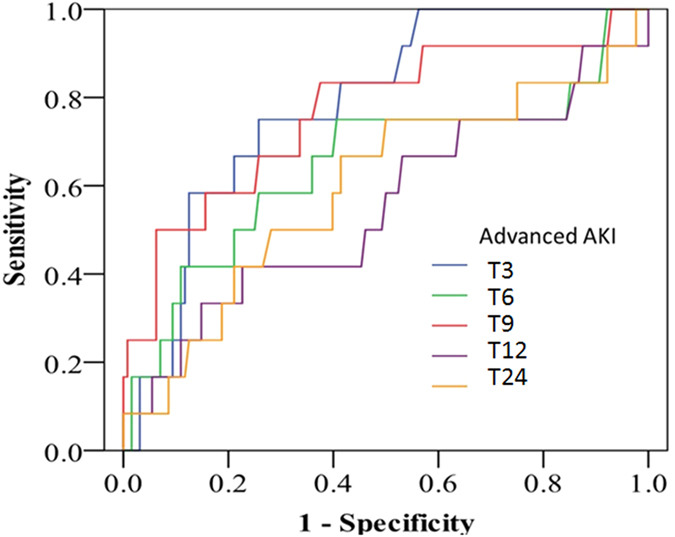
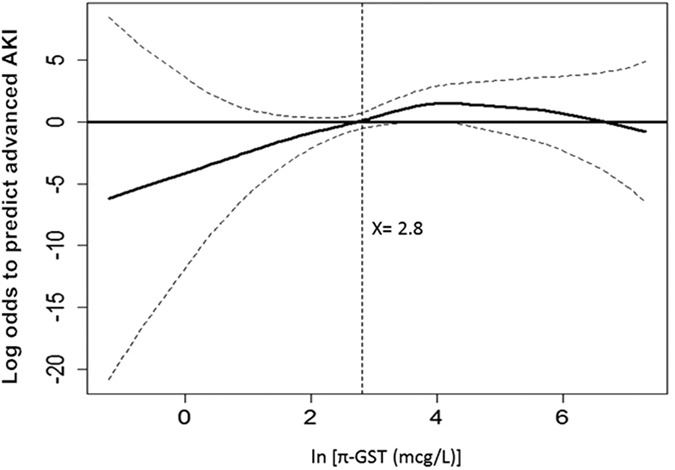
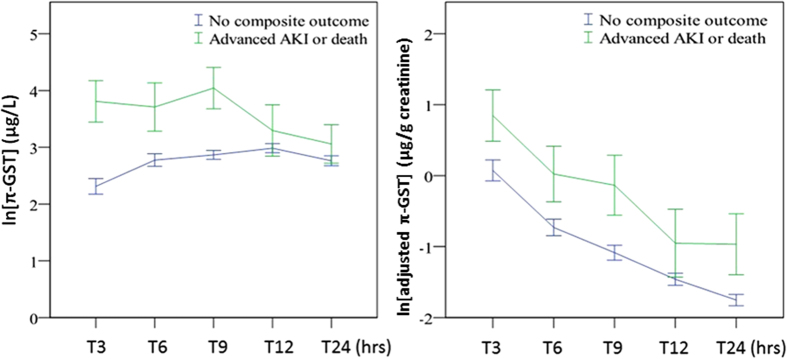
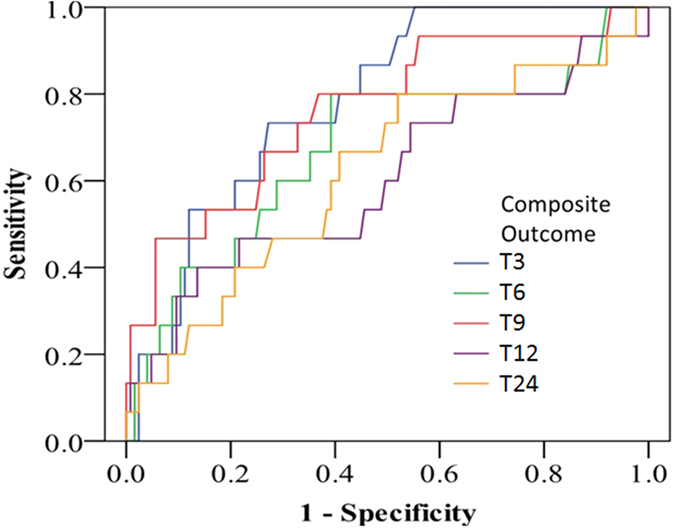
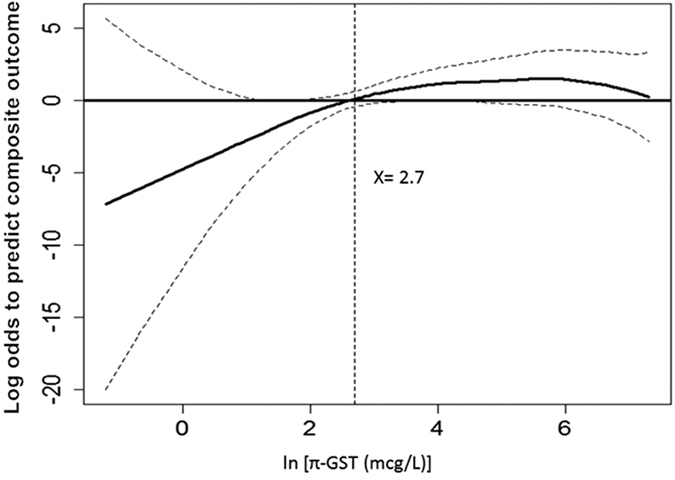
Urinary biomarkers augment the diagnosis of acute kidney injury (AKI), with AKI after cardiovascular surgeries being a prototype of prognosis scenario. Glutathione S-transferases (GST) were evaluated as biomarkers of AKI. Urine samples were collected in 141 cardiovascular surgical patients and analyzed for urinary alpha-(α-) and pi-(π-) GSTs. The outcomes of advanced AKI (KDIGO stage 2, 3) and all-cause in-patient mortality, as composite outcome, were recorded. Areas under the receiver operator characteristic (ROC) curves and multivariate generalized additive model (GAM) were applied to predict outcomes. Thirty-eight (26.9%) patients had AKI, while 12 (8.5%) were with advanced AKI. Urinary π-GST differentiated patients with/without advanced AKI or composite outcome after surgery (p < 0.05 by generalized estimating equation). Urinary π-GST predicted advanced AKI at 3 hrs post-surgery (p = 0.033) and composite outcome (p = 0.009), while the corresponding ROC curve had AUC of 0.784 and 0.783. Using GAM, the cutoff value of 14.7 μg/L for π-GST showed the best performance to predict composite outcome. The addition of π-GST to the SOFA score improved risk stratification (total net reclassification index = 0.47). Thus, urinary π-GST levels predict advanced AKI or hospital mortality after cardiovascular surgery and improve in SOFA outcome assessment specific to AKI.
Conflict of interest statement
The human alpha GST and piGST assays were performed by Rory Connolly, R&D Scientist at EKF Diagnostics. No other potential conflicts of interest relevant to this article were reported.
Figures
References
-
- Siew E. D., Ware L. B. & Ikizler T. A. Biological markers of acute kidney injury. J Am Soc Nephrol 22, 810–820 (2011). - PubMed
-
- Mishra J. Identification of Neutrophil Gelatinase-Associated Lipocalin as a Novel Early Urinary Biomarker for Ischemic Renal Injury. J Am Soc Nephrol 14, 2534–2543 (2003). - PubMed
-
- Mishra J. et al.. Neutrophil gelatinase-associated lipocalin (NGAL) as a biomarker for acute renal injury after cardiac surgery. The Lancet 365, 1231–1238 (2005). - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
