

Impact of Hepatitis C Virus/Schistosoma mansoni Coinfection on the Circulating Levels of HCV-NS4 Protein and Extracellular-Matrix Deposition in Patients with Different Hepatic Fibrosis Stages
- PMID: 27527625
- PMCID: PMC5094215
- DOI: 10.4269/ajtmh.16-0129
Impact of Hepatitis C Virus/Schistosoma mansoni Coinfection on the Circulating Levels of HCV-NS4 Protein and Extracellular-Matrix Deposition in Patients with Different Hepatic Fibrosis Stages
Abstract
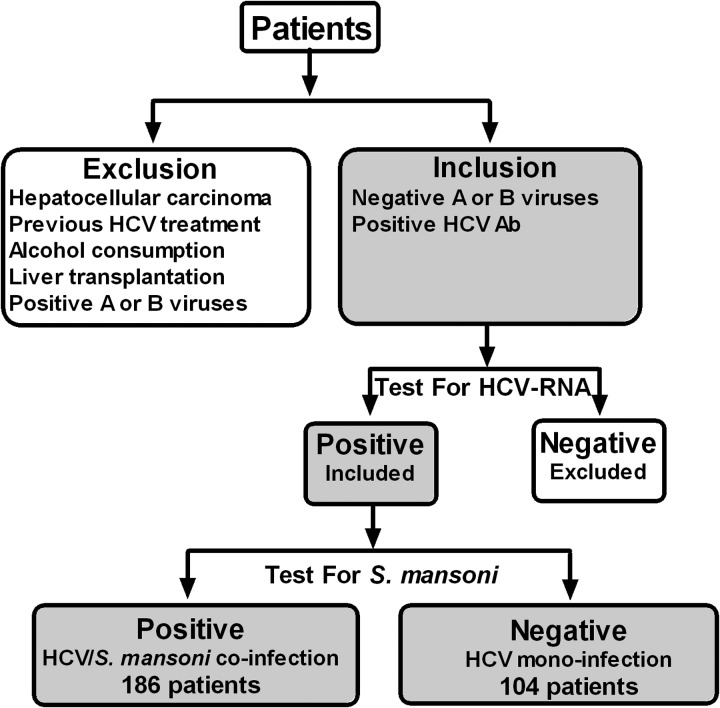
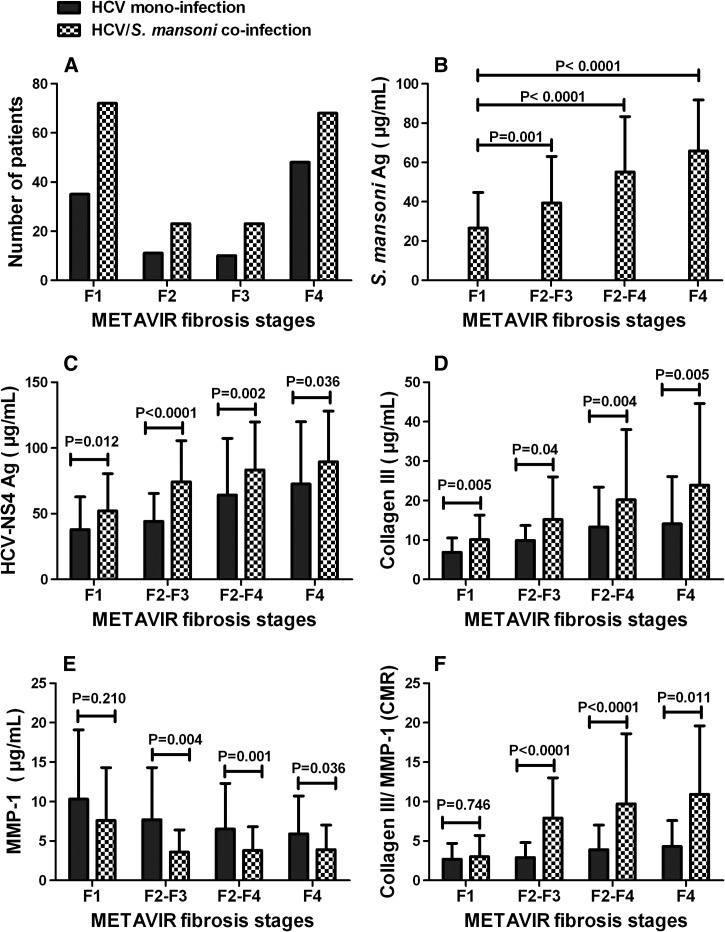
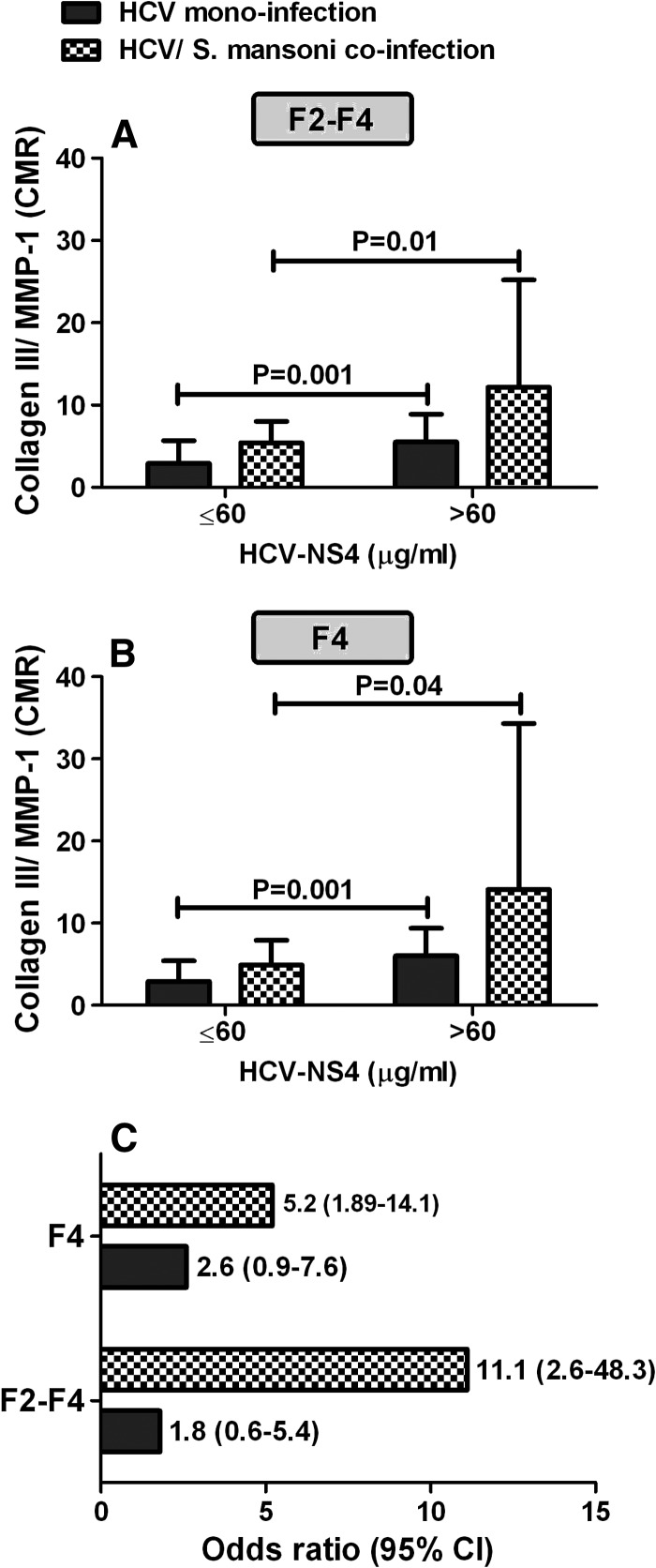
Hepatitis C virus (HCV)/Schistosoma mansoni coinfection is common in Egypt and other developing countries. This study aimed to investigate the influence of HCV/S. mansoni coinfection on the concentration of HCV-nonstructural protein-4 (NS4) in addition to collagen III and matrix metalloproteinase-1 (MMP-1) in different hepatic fibrosis stages. We found that coinfected patients (N = 186) showed significantly (P < 0.05, Mann-Whitney U test) higher concentrations of HCV-NS4, collagen III, and collagen III/MMP-1 ratio (CMR) than those with HCV monoinfection (N = 104) in different fibrosis stages. Conversely, coinfected patients showed significantly lower concentrations of MMP-1 when compared with HCV monoinfection. The elevated levels of CMR in case of HCV monoinfection yielded an estimated odds ratio of 1.8 and 2.6 for developing significant fibrosis (F2-F4) and cirrhosis (F4), respectively. HCV/S. mansoni coinfection increased the risk for developing F2-F4 and F4 several fold yielding an estimated odds ratio of 11.1 and 5.2, respectively. This means that coinfected patients have a 6-fold and 2-fold increased risk of developing F2-F4 and F4, respectively, over HCV-monoinfected patients. Thus, elevated levels of HCV-NS4 and CMR in HCV/S. mansoni coinfection suggest increased susceptibility of coinfected patients, compared with those with HCV monoinfection, for accelerating hepatic fibrosis progression.
© The American Society of Tropical Medicine and Hygiene.
Figures
References
-
- European Association for Study of Liver EASL Clinical Practice Guidelines: management of hepatitis C virus infection. J Hepatol. 2014;60:392–420. - PubMed
-
- Negro F. Curbing hepatitis C virus spread in Egypt. Lancet Glob Health. 2014;2:e495–e496. - PubMed
-
- Lavanchy D. Evolving epidemiology of hepatitis C virus. Clin Microbiol Infect. 2011;17:107–115. - PubMed
-
- Gryseels B. Schistosomiasis. Infect Dis Clin North Am. 2012;26:383–397. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
