

The Association of Surgical Margins and Local Recurrence in Women with Ductal Carcinoma In Situ Treated with Breast-Conserving Therapy: A Meta-Analysis
- PMID: 27527715
- PMCID: PMC5160992
- DOI: 10.1245/s10434-016-5446-2
The Association of Surgical Margins and Local Recurrence in Women with Ductal Carcinoma In Situ Treated with Breast-Conserving Therapy: A Meta-Analysis
Abstract
Purpose: There is no consensus on adequate negative margins in breast-conserving surgery (BCS) for ductal carcinoma in situ (DCIS). We systematically reviewed the evidence on margins in BCS for DCIS.
Methods: A study-level meta-analysis of local recurrence (LR), microscopic margin status and threshold distance for negative margins. LR proportion was modeled using random-effects logistic meta-regression (frequentist) and network meta-analysis (Bayesian) that allows for multiple margin distances per study, adjusting for follow-up time.
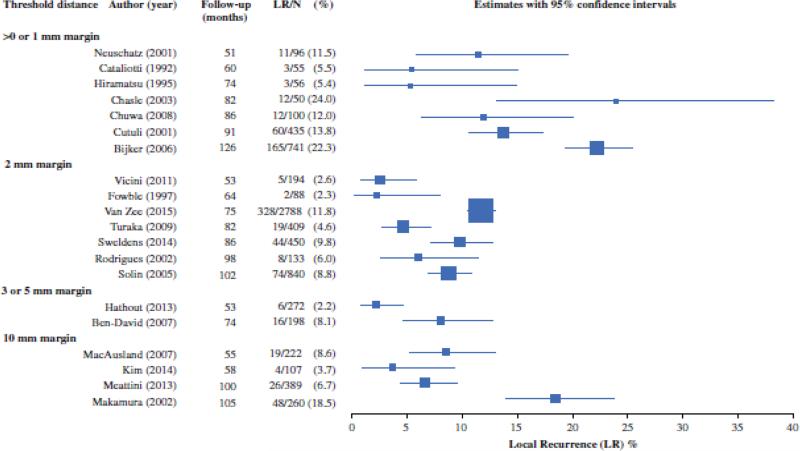
Results: Based on 20 studies (LR: 865 of 7883), odds of LR were associated with margin status [logistic: odds ratio (OR) 0.53 for negative vs. positive/close (p < 0.001); network: OR 0.45 for negative vs. positive]. In logistic meta-regression, relative to >0 or 1 mm, ORs for 2 mm (0.51), 3 or 5 mm (0.42) and 10 mm (0.60) showed comparable significant reductions in the odds of LR. In the network analysis, ORs relative to positive margins for 2 (0.32), 3 (0.30) and 10 mm (0.32) showed similar reductions in the odds of LR that were greater than for >0 or 1 mm (0.45). There was weak evidence of lower odds at 2 mm compared with >0 or 1 mm [relative OR (ROR) 0.72, 95 % credible interval (CrI) 0.47-1.08], and no evidence of a difference between 2 and 10 mm (ROR 0.99, 95 % CrI 0.61-1.64). Adjustment for covariates, and analyses based only on studies using whole-breast radiotherapy, did not change the findings.
Conclusion: Negative margins in BCS for DCIS reduce the odds of LR; however, minimum margin distances above 2 mm are not significantly associated with further reduced odds of LR in women receiving radiation.
Figures
References
-
- Virnig BA, Tuttle TM, Shamliyan T, Kane RL. Ductal carcinoma in Situ of the breast: A systematic review of incidence, treatment, and outcomes. J Natl Cancer Inst. 2010;102:170–178. - PubMed
-
- Irwig L, Bennetts A. Quality of life after breast conservation or mastectomy: A systematic review. Aust New Zealand J Surg. 1997;67:750–754. - PubMed
-
- Dunne C, Burke JP, Morrow M, Kell MR. Effect of margin status on local recurrence after breast conservation and radiation therapy for ductal carcinoma in situ. J Clin Oncol. 2009;27:1615–1620. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
