

Autonomic Blockade Reverses Endothelial Dysfunction in Obesity-Associated Hypertension
- PMID: 27528067
- PMCID: PMC5016238
- DOI: 10.1161/HYPERTENSIONAHA.116.07681
Autonomic Blockade Reverses Endothelial Dysfunction in Obesity-Associated Hypertension
Abstract
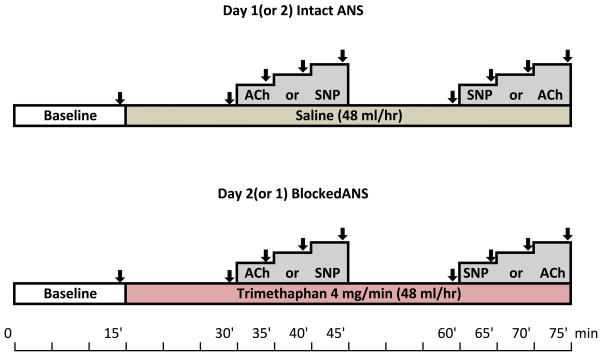
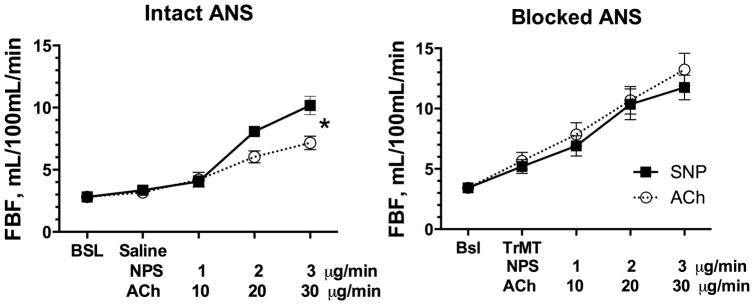
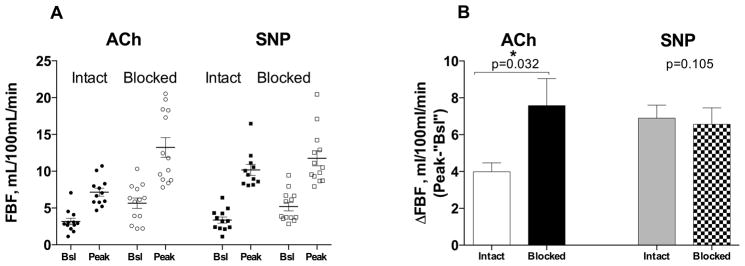
Impaired nitric oxide (NO) vasodilation (endothelial dysfunction) is associated with obesity and thought to be a factor in the development of hypertension. We previously found that NO synthesis inhibition had similar pressor effects in obese hypertensives compared with healthy control during autonomic blockade, suggesting that impaired NO vasodilation is secondary to sympathetic activation. We tested this hypothesis by determining the effect of autonomic blockade (trimethaphan 4 mg/min IV) on NO-mediated vasodilation (increase in forearm blood flow to intrabrachial acetylcholine) compared with endothelial-independent vasodilation (intrabrachial sodium nitroprusside) in obese hypertensive subjects (30<body mass index<40 kg/m(2)). Acetylcholine and sodium nitroprusside were given at equipotent doses (10, 30, and 50 μg/min and 1, 2, and 3 μg/min, respectively) to 14 obese subjects (49±3.6 years, 34±1 kg/m(2), 165/94±7/6 mm Hg), on separate occasions 1 month apart, randomly assigned. Autonomic blockade increased basal forearm blood flow (from 3.9±0.7 to 5.2±1.2 mL/100 mL per minute, P=0.078). As expected, NO-mediated vasodilation was blunted on the intact day compared with NO-independent vasodilation; forearm blood flow increased from 3.6±0.6 to 10.1±1.1 with the highest dose of nitroprusside, but only from 3.7±0.4 to 7.2±0.8 mL/100 mL per minute with the highest dose of acetylcholine, P<0.05. In contrast, forearm blood flow responses to acetylcholine were restored by autonomic blockade and were no longer different to nitroprusside (from 6.2±1.1 to 11.4±1.6 mL/100 mL per minute and from 5.2±0.9 to 12.5±0.9, respectively, P=0.58). Our results support the concept that sympathetic activation contributes to the impairment in NO-mediated vasodilation seen in obesity-associated hypertension and provides further rationale to explore it as a therapeutic target.
Keywords: autonomic nervous system; hypertension; nitric oxide; obesity; vasodilation.
© 2016 American Heart Association, Inc.
Conflict of interest statement
Conflict(s) of Interest/Disclosure(s): None
Figures
References
-
- Narkiewicz K, van de Borne PJ, Cooley RL, Dyken ME, Somers VK. Sympathetic activity in obese subjects with and without obstructive sleep apnea. Circulation. 1998;98:772–776. - PubMed
-
- Weyer C, Pratley RE, Snitker S, Spraul M, Ravussin E, Tataranni PA. Ethnic differences in insulinemia and sympathetic tone as links between obesity and blood pressure. HTN. 2000;36:531–537. - PubMed
-
- Ozata M, Ozdemir IC, Licinio J. Human leptin deficiency caused by a missense mutation: Multiple endocrine defects, decreased sympathetic tone, and immune system dysfunction indicate new targets for leptin action, greater central than peripheral resistance to the effects of leptin, and spontaneous correction of leptin-mediated defects. J Clin Endocrinol Metab. 1999;84:3686–3695. - PubMed
-
- Rumantir MS, Vaz M, Jennings GL, Collier G, Kaye DM, Seals DR, Wiesner GH, Brunner-La Rocca HP, Esler MD. Neural mechanisms in human obesity-related hypertension. J Hypertens. 1999;17:1125–1133. - PubMed
-
- Vaz M, Jennings G, Turner A, Cox H, Lambert G, Esler M. Regional sympathetic nervous activity and oxygen consumption in obese normotensive human subjects. Circulation. 1997;96:3423–3429. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
