

Pediatric stress fractures: a pictorial essay
- PMID: 27528851
- PMCID: PMC4910803
Pediatric stress fractures: a pictorial essay
Abstract
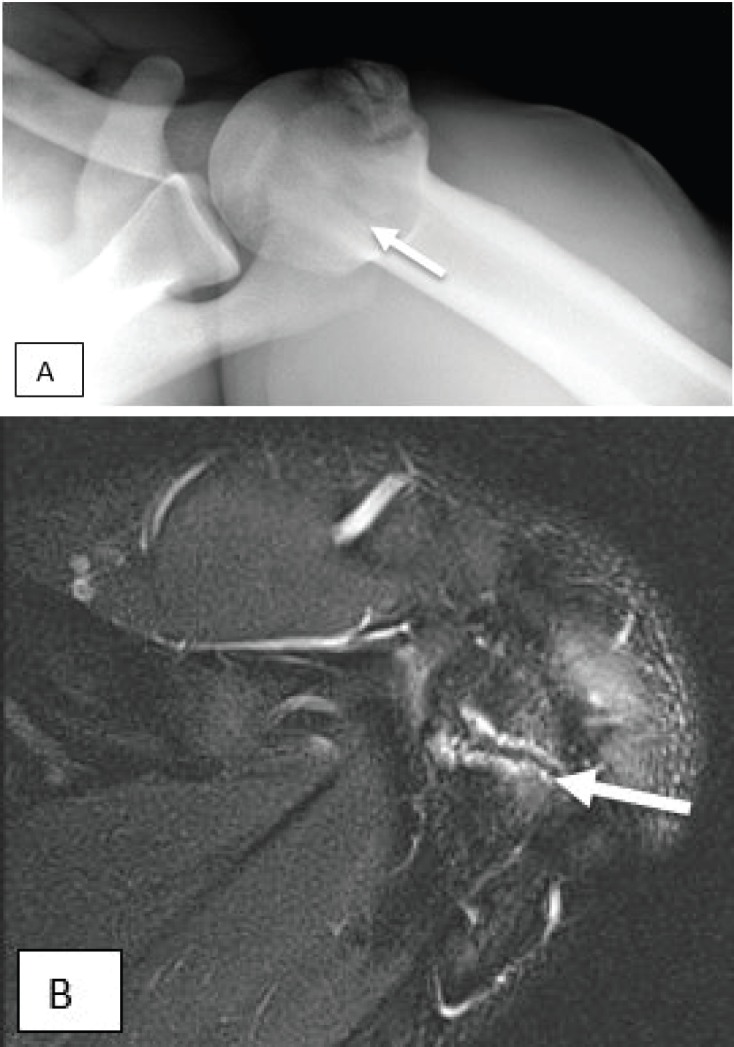
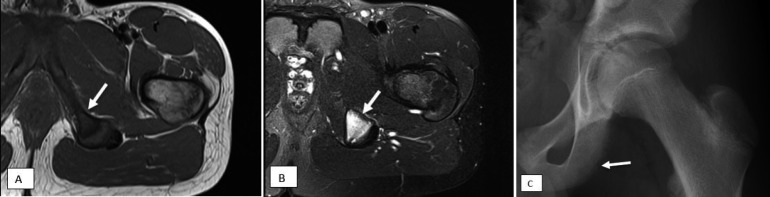
More children are participating in organized and recreational athletics at a younger age. It has been well documented that increased athletic specialization and year-round activities have resulted in higher incidences of overuse injuries, including stress fractures and stress reactions. Initially, stress fractures can be radiographically occult. Continued stress on the injured bone or cartilage can lead to progressive radiographic changes. Because of the prevalence of these injuries, both orthopedic surgeons and radiologists should be aware of the radiographic and magnetic resonance imaging (MRI) features of common stress fractures in children. This article reviews frequently encountered stress fractures involving various bones in the pediatric population.
Figures













References
-
- Anderson MW, Greenspan A. Stress fractures. Radiology. 1996 Apr;199(1):1–12. - PubMed
-
- Jaimes C, Jimenez M, Shabshin N, Laor T, Jaramillo D. Taking the stress out of evaluating stress injuries in children. Radiographics. 2012 Mar-Apr;32(2):537–55. - PubMed
-
- Jones BH, Harris JM, Vinh TN, Rubin C. Exercise induced stress fractures and stress reactions of bone: epidemiology, etiology, and classification. Exerc Sport Sci Rev. 1989;17:379–422. - PubMed
-
- Laor T, Wall EJ, Vu LP. Physeal widening in the knee due to stress injury in child athletes. AJR Am J Roentgenol. 2006;186(5):1260–4. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources