

Clinically integrated multi-organ point-of-care ultrasound for undifferentiated respiratory difficulty, chest pain, or shock: a critical analytic review
- PMID: 27529030
- PMCID: PMC4983789
- DOI: 10.1186/s40560-016-0172-1
Clinically integrated multi-organ point-of-care ultrasound for undifferentiated respiratory difficulty, chest pain, or shock: a critical analytic review
Abstract
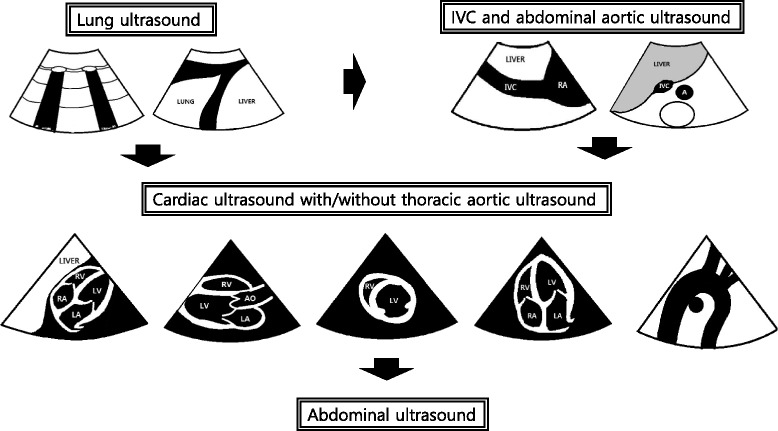
Rapid and accurate diagnosis and treatment are paramount in the management of the critically ill. Critical care ultrasound has been widely used as an adjunct to standard clinical examination, an invaluable extension of physical examination to guide clinical decision-making at bedside. Recently, there is growing interest in the use of multi-organ point-of-care ultrasound (MOPOCUS) for the management of the critically ill, especially in the early phase of resuscitation. This article will review the role and utility of symptom-based and sign-oriented MOPOCUS in patients with undifferentiated respiratory difficulty, chest pain, or shock and how it can be performed in a timely, effective, and efficient manner.
Keywords: Chest pain; Multi-organ point-of-care ultrasound; Respiratory difficulty; Shock.
Figures


Similar articles
-
Bedside lung ultrasound in the care of the critically ill.Crit Care Resusc. 2017 Dec;19(4):327-336. Crit Care Resusc. 2017. PMID: 29202259
-
Point-of-Care Lung Ultrasound in Critically ill Patients.Rev Recent Clin Trials. 2018 Jan 31;13(1):15-26. doi: 10.2174/1574887112666170911125750. Rev Recent Clin Trials. 2018. PMID: 28901850 Review.
-
Lung ultrasound in a Singapore COVID-19 intensive care unit patient and a review of its potential clinical utility in pandemic.J Ultrason. 2020;20(81):e154-e158. doi: 10.15557/JoU.2020.0025. Epub 2020 Jun 15. J Ultrason. 2020. PMID: 32609971 Free PMC article.
-
Sepsis Care Pathway 2019.Qatar Med J. 2019 Nov 7;2019(2):4. doi: 10.5339/qmj.2019.qccc.4. eCollection 2019. Qatar Med J. 2019. PMID: 31763206 Free PMC article.
-
Point-of-care ultrasound with pocket-size devices in emergency department.Echocardiography. 2019 Sep;36(9):1755-1764. doi: 10.1111/echo.14451. Epub 2019 Aug 8. Echocardiography. 2019. PMID: 31393640 Review.
Cited by
-
It's Not All about Echocardiography. Open the Lung Window for the Cardiac Emergencies.Medicina (Kaunas). 2021 Jan 14;57(1):69. doi: 10.3390/medicina57010069. Medicina (Kaunas). 2021. PMID: 33466680 Free PMC article. Review.
-
The Role of Point-of-Care Ultrasound in the Emergency Department: The Case of a Contained Rupture of the Ascending Aorta Due to Type A Dissection Causing Subacute Cardiac Tamponade.CASE (Phila). 2022 Aug 15;6(6):275-280. doi: 10.1016/j.case.2022.05.005. eCollection 2022 Aug. CASE (Phila). 2022. PMID: 36036050 Free PMC article.
-
Echocardiographic Assessment of Patients with Pulmonary Tumor Thrombotic Microangiopathy First Diagnosed in the Emergency Department.Diagnostics (Basel). 2022 Jan 20;12(2):259. doi: 10.3390/diagnostics12020259. Diagnostics (Basel). 2022. PMID: 35204350 Free PMC article.
-
Clinical Guidance for Point-of-Care Ultrasound in the Emergency and Critical Care Areas after Implementing Insurance Coverage in Korea.J Korean Med Sci. 2020 Feb 24;35(7):e54. doi: 10.3346/jkms.2020.35.e54. J Korean Med Sci. 2020. PMID: 32080988 Free PMC article. Review.
-
Review of simulation model for education of point-of-care ultrasound using easy-to-make tools.World J Clin Cases. 2020 Oct 6;8(19):4286-4302. doi: 10.12998/wjcc.v8.i19.4286. World J Clin Cases. 2020. PMID: 33083388 Free PMC article. Review.
References
-
- Labovitz AJ, Noble VE, Bierig M, Goldstein SA, Jones R, Kort S, et al. Focused cardiac ultrasound in the emergent setting: a consensus statement of the American Society of Echocardiography and American College of Emergency Physicians. J Am Soc Echocardiogr. 2010;23(12):1225–30. doi: 10.1016/j.echo.2010.10.005. - DOI - PubMed
-
- Kajimoto K, Madeen K, Nakayama T, Tsudo H, Kuroda T, Abe T. Rapid evaluation by lung-cardiac-inferior vena cava (LCI) integrated ultrasound for differentiating heart failure from pulmonary disease as the cause of acute dyspnea in the emergency setting. Cardiovasc Ultrasound. 2012;10(1):49. doi: 10.1186/1476-7120-10-49. - DOI - PMC - PubMed
-
- Laursen CB, Sloth E, Lassen AT, Christensen RD, Lambrechtsen J, Madsen PH, et al. Focused sonographic examination of the heart, lungs and deep veins in an unselected population of acute admitted patients with respiratory symptoms: a protocol for a prospective, blinded, randomised controlled trial. BMJ open. 2012;2(3). Pubmed Central PMCID: PMC3367153. Epub 2012/06/01. eng - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
