

Neuroimaging findings in acute pediatric diabetic ketoacidosis
- PMID: 27531862
- PMCID: PMC5033105
- DOI: 10.1177/1971400916665389
Neuroimaging findings in acute pediatric diabetic ketoacidosis
Abstract
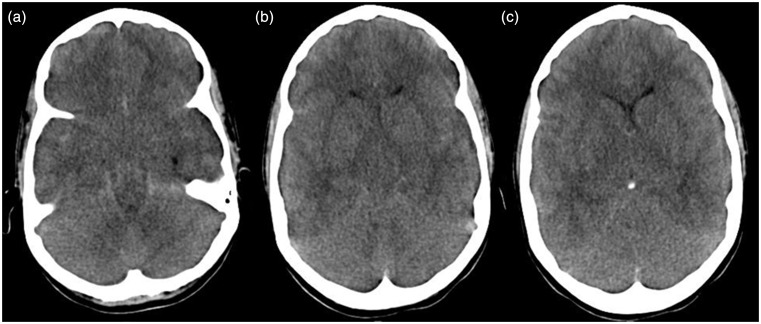
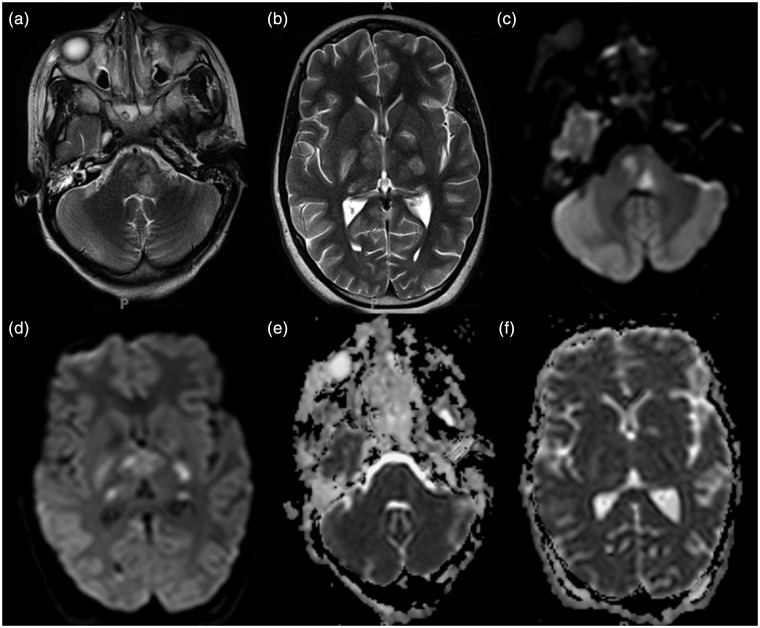
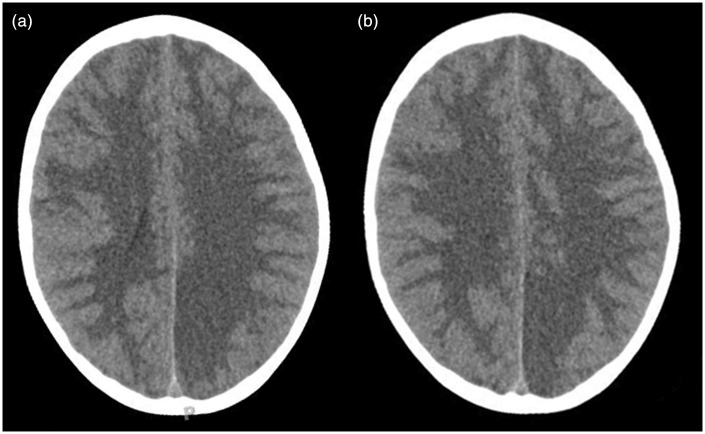
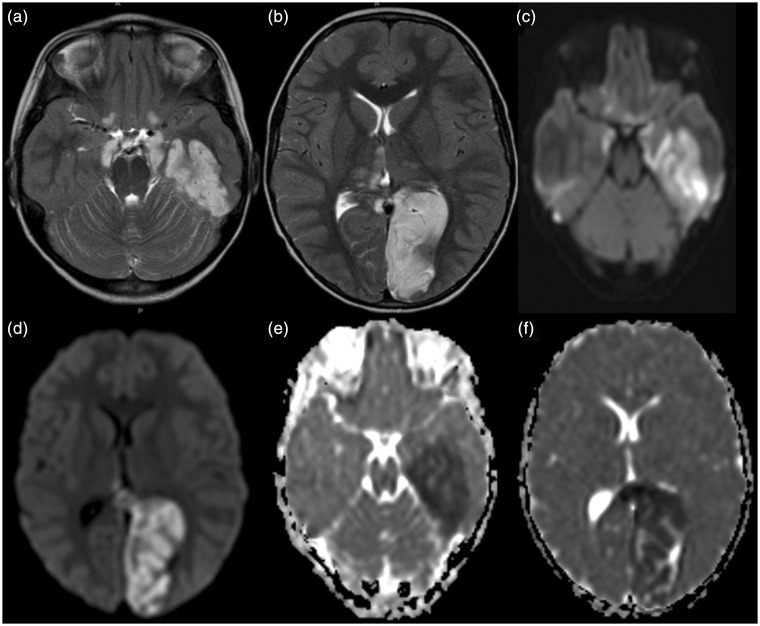
Diabetic ketoacidosis (DKA) is a state of severe insulin deficiency and a serious complication in children with diabetes mellitus type 1. In a small number of children, DKA is complicated by injury of the central nervous system. These children have a significant mortality and high long-term neurological morbidity. Cerebral edema is the most common neuroimaging finding in children with DKA and may cause brain herniation. Ischemic or hemorrhagic stroke during the acute DKA episode is less common and accounts for approximately 10% of intracerebral complications of DKA. Here we present the neuroimaging findings of two children with DKA and brain injury. Familiarity with the spectrum of neuroimaging findings seen in pediatric DKA is important to allow early detection as well as initiation of therapy and, hence, prevent complications of the central nervous system.
Keywords: Diabetic ketoacidosis; MRI; brain; children; stroke.
© The Author(s) 2016.
Figures
Similar articles
-
Diabetic ketoacidosis with central nervous system involvement: Conventional and advanced magnetic resonance neuroimaging findings.Neuroradiol J. 2025 Apr;38(2):247-250. doi: 10.1177/19714009241248745. Epub 2024 Apr 23. Neuroradiol J. 2025. PMID: 38654625 Free PMC article.
-
Symptomatic cerebral infarction in a child with severe diabetic ketoacidosis.J Pediatr Endocrinol Metab. 2014 Sep;27(9-10):1001-4. doi: 10.1515/jpem-2014-0037. J Pediatr Endocrinol Metab. 2014. PMID: 24825089
-
Diabetic ketoacidosis. Neurologic collapse during treatment followed by severe developmental morbidity.Clin Pediatr (Phila). 1990 Aug;29(8):451-6. doi: 10.1177/000992289002900807. Clin Pediatr (Phila). 1990. PMID: 1698585
-
Diabetic ketoacidosis in the pediatric emergency department.Emerg Med Clin North Am. 2013 Aug;31(3):755-73. doi: 10.1016/j.emc.2013.05.004. Epub 2013 Jul 6. Emerg Med Clin North Am. 2013. PMID: 23915602 Review.
-
Diabetic ketoacidosis in the pediatric ICU.Pediatr Clin North Am. 2008 Jun;55(3):577-87, x. doi: 10.1016/j.pcl.2008.02.015. Pediatr Clin North Am. 2008. PMID: 18501755 Review.
Cited by
-
Glycaemic Imbalances in Seizures and Epilepsy of Paediatric Age: A Literature Review.J Clin Med. 2023 Mar 29;12(7):2580. doi: 10.3390/jcm12072580. J Clin Med. 2023. PMID: 37048663 Free PMC article. Review.
-
Ischaemic Haemorrhagic Stroke in a Child with New Onset Type 1 Diabetes Mellitus.Eur Endocrinol. 2018 Apr;14(1):59-61. doi: 10.17925/EE.2018.14.1.59. Epub 2018 Apr 18. Eur Endocrinol. 2018. PMID: 29922355 Free PMC article.
-
Cerebral oedema and dural sinus thrombosis in an adolescent with diabetic ketoacidosis.BMJ Case Rep. 2021 Apr 9;14(4):e241690. doi: 10.1136/bcr-2021-241690. BMJ Case Rep. 2021. PMID: 33837035 Free PMC article. No abstract available.
-
Reversible global hypoperfusion in an adult patient with a mixed diabetic ketoacidosis/hyperglycemic hyperosmolar coma: A case report.Clin Case Rep. 2022 Apr 4;10(4):e05576. doi: 10.1002/ccr3.5576. eCollection 2022 Apr. Clin Case Rep. 2022. PMID: 35414918 Free PMC article.
-
Diabetic ketoacidosis and cerebral edema: a rare case of infarct-like MRI findings in a pediatric patient.Ann Med Surg (Lond). 2025 May 12;87(6):3963-3968. doi: 10.1097/MS9.0000000000003332. eCollection 2025 Jun. Ann Med Surg (Lond). 2025. PMID: 40486604 Free PMC article.
References
-
- Olivieri L, Chasm R. Diabetic ketoacidosis in the pediatric emergency department. Emerg Med Clin North Am 2013; 31: 755–773. - PubMed
-
- Wolfsdorf JI. The International Society of Pediatric and Adolescent Diabetes guidelines for management of diabetic ketoacidosis: Do the guidelines need to be modified? Pediatr Diabetes 2014; 15: 277–286. - PubMed
-
- Wootton-Gorges SL, Glaser NS. Imaging of the brain in children with type I diabetes mellitus. Pediatr Radiol 2007; 37: 863–869. - PubMed
-
- Roe TF, Crawford TO, Huff KR, et al. Brain infarction in children with diabetic ketoacidosis. J Diabetes Complications 1996; 10: 100–108. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
