

A hypofractionated radiation regimen avoids the lymphopenia associated with neoadjuvant chemoradiation therapy of borderline resectable and locally advanced pancreatic adenocarcinoma
- PMID: 27532020
- PMCID: PMC4986363
- DOI: 10.1186/s40425-016-0149-6
A hypofractionated radiation regimen avoids the lymphopenia associated with neoadjuvant chemoradiation therapy of borderline resectable and locally advanced pancreatic adenocarcinoma
Abstract
Background: Preclinical studies have shown synergy between radiation therapy and immunotherapy. However, in almost all preclinical models, radiation is delivered in single doses or short courses of high doses (hypofractionated radiation). By contrast in most clinical settings, radiation is delivered as standard small daily fractions of 1.8-2 Gy to achieve total doses of 50-54 Gy (fractionated radiation). We do not yet know the optimal dose and scheduling of radiation for combination with chemotherapy and immunotherapy.
Methods: To address this, we analyzed the effect of neoadjuvant standard fractionated and hypofractionated chemoradiation on immune cells in patients with locally advanced and borderline resectable pancreatic adenocarcinoma.
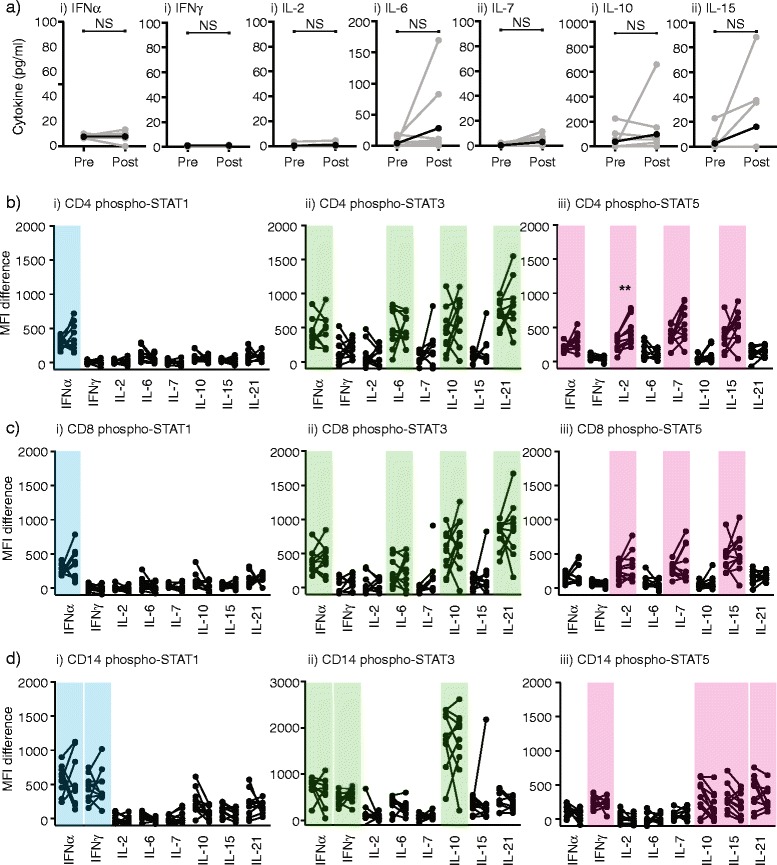
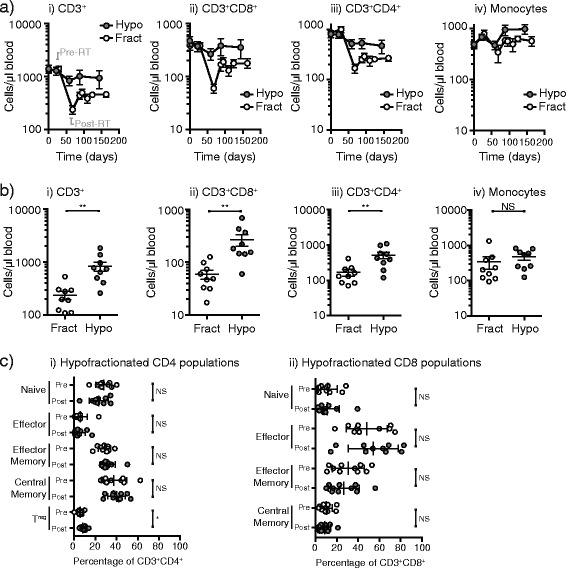
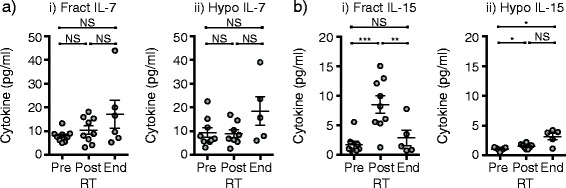
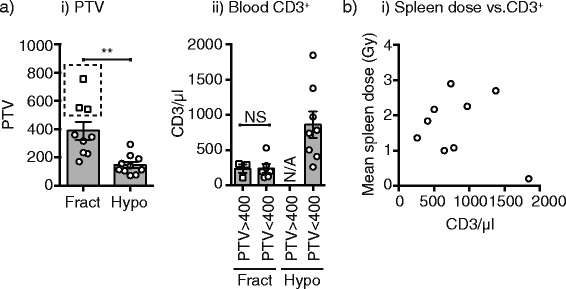
Results: We found that standard fractionated chemoradiation resulted in a significant and extended loss of lymphocytes that was not explained by a lack of homeostatic cytokines or response to cytokines. By contrast, treatment with hypofractionated radiation therapy avoided the loss of lymphocytes associated with conventional fractionation.
Conclusion: Hypofractionated neoadjuvant chemoradiation is associated with reduced systemic loss of T cells.
Trial registration: ClinicalTrials.gov NCT01342224, April 21, 2011; NCT01903083, July 2, 2013.
Keywords: Chemotherapy; Fractionation; Gemcitabine; Homeostatic repopulation; IL-15; IL-7; Immunotherapy; Lymphocytes; Lymphodepletion; Radiation.
Figures

References
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous