

In-airway molecular flow sensing: A new technology for continuous, noninvasive monitoring of oxygen consumption in critical care
- PMID: 27532048
- PMCID: PMC4980105
- DOI: 10.1126/sciadv.1600560
In-airway molecular flow sensing: A new technology for continuous, noninvasive monitoring of oxygen consumption in critical care
Abstract
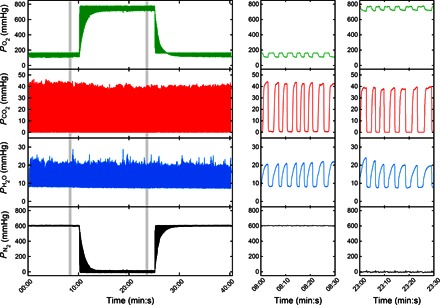
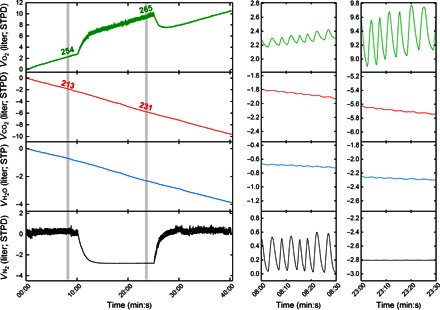
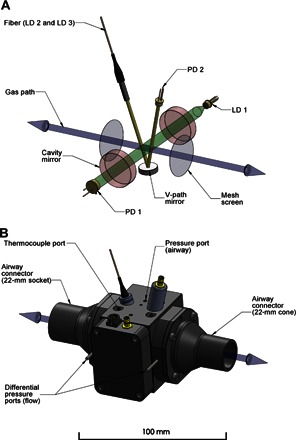
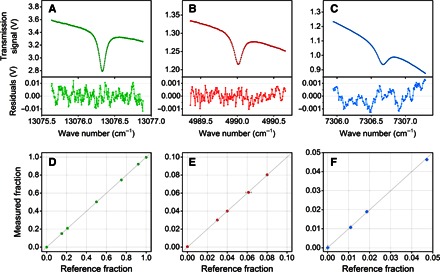
There are no satisfactory methods for monitoring oxygen consumption in critical care. To address this, we adapted laser absorption spectroscopy to provide measurements of O2, CO2, and water vapor within the airway every 10 ms. The analyzer is integrated within a novel respiratory flow meter that is an order of magnitude more precise than other flow meters. Such precision, coupled with the accurate alignment of gas concentrations with respiratory flow, makes possible the determination of O2 consumption by direct integration over time of the product of O2 concentration and flow. The precision is illustrated by integrating the balance gas (N2 plus Ar) flow and showing that this exchange was near zero. Measured O2 consumption changed by <5% between air and O2 breathing. Clinical capability was illustrated by recording O2 consumption during an aortic aneurysm repair. This device now makes easy, accurate, and noninvasive measurement of O2 consumption for intubated patients in critical care possible.
Keywords: Gas lasers; absorbence spectroscopy; gas exchange; laser spectroscopy; medical device; medical technology; oxygen consumption; respiration.
Figures


References
-
- Black C., Grocott M. P. W., Singer M., Metabolic monitoring in the intensive care unit: A comparison of the Medgraphics Ultima, Deltatrac II, and Douglas bag collection methods. Br. J. Anaesth. 114, 261–268 (2015). - PubMed
-
- Robinson P. D., Latzin P., Verbanck S., Hall G. L., Horsley A., Gappa M., Thamrin C., Arets H. G. M., Aurora P., Fuchs S. I., King G. G., Lum S., Macleod K., Paiva M., Pillow J. J., Ranganathan S., Ranganathan S., Ratjen F., Singer F., Sonnappa S., Stocks J., Subbarao P., Thompson B. R., Gustafsson P. M., Consensus statement for inert gas washout measurement using multiple- and single- breath tests. Eur. Respir. J. 41, 507–522 (2013). - PubMed
-
- Arieli R., Mass spectrometer for respiratory research. Respir. Physiol. Neurobiol. 170, 183–184 (2010). - PubMed
-
- Finucane K. E., Egan B. A., Dawson S. V., Linearity and frequency response of pneumotachographs. J. Appl. Physiol. 32, 121–126 (1972). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
