

Long term outcome and side effects in patients receiving low-dose I125 brachytherapy: a retrospective analysis
- PMID: 27532118
- PMCID: PMC5066886
- DOI: 10.1590/S1677-5538.IBJU.2015.0542
Long term outcome and side effects in patients receiving low-dose I125 brachytherapy: a retrospective analysis
Abstract
Objectives: To retrospectively evaluate the disease free survival (DFS),disease specific survival (DSS),overall survival (OS) and side effects in patients who received low-dose rate (LDR) brachytherapy with I125 stranded seeds.
Materials and methods: Between july 2003 and august 2012, 274 patients with organ confined prostate cancer were treated with permanent I125 brachytherapy. The median follow-up, age and pretreatment prostate specific antigen (iPSA) was 84 months (12-120), 67 years (50-83) and 7.8 ng/mL (1.14-38), respectively. Median Gleason score was 6 (3-9). 219 patients (80%) had stage cT1c, 42 patients (15.3%) had stage cT2a, 3 (1.1%) had stage cT2b and 3 (1.1%) had stage cT2c. The median D90 was 154.3 Gy (102.7-190.2).
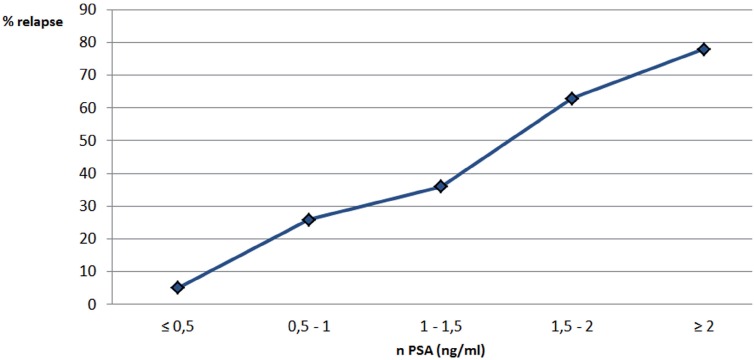
Results: DSS was 98.5%.OS was 93.5%. 13 patients (4.7%) developed systemic disease, 7 patients (2.55%) had local progression. In 139 low risk patients, the 5 year biochemical freedom from failure rate (BFFF) was 85% and 9 patients (6.4%) developed clinical progression. In the intermediate risk group, the 5 year BFFF rate was 70% and 5 patients (7.1%) developed clinical progression. Median nPSA in patients with biochemical relapse was 1.58 ng/mL (0.21 - 10.46), median nPSA in patients in remission was 0.51 ng/mL (0.01 - 8.5). Patients attaining a low PSA nadir had a significant higher BFFF (p<0.05). Median D90 in patients with biochemical relapse was 87.2 Gy (51 - 143,1). Patients receiving a high D90 had a significant higher BFFF (p<0.05).
Conclusion: In a well selected patient population, LDR brachytherapy offers excelente outcomes. Reaching a low PSA nadir and attaining high D90 values are significant predictors for a higher DFS.
Keywords: Brachytherapy; Prostate-Specific Antigen; Prostatic Neoplasms.
Copyright® by the International Brazilian Journal of Urology.
Conflict of interest statement
Conflicts of Interest: None declared.
Figures

Similar articles
-
PSA nadir of <0.5 ng/mL following brachytherapy for early-stage prostate adenocarcinoma is associated with freedom from prostate-specific antigen failure.Int J Radiat Oncol Biol Phys. 2012 Jun 1;83(2):600-7. doi: 10.1016/j.ijrobp.2011.07.009. Epub 2011 Oct 8. Int J Radiat Oncol Biol Phys. 2012. PMID: 21985944
-
Multi-institutional analysis of long-term outcome for stages T1-T2 prostate cancer treated with permanent seed implantation.Int J Radiat Oncol Biol Phys. 2007 Feb 1;67(2):327-33. doi: 10.1016/j.ijrobp.2006.08.056. Epub 2006 Nov 2. Int J Radiat Oncol Biol Phys. 2007. PMID: 17084558
-
Dosimetry doesn't seem to predict the control of organ-confined prostate cancer after I-125 brachytherapy. Evaluation in 150 patients.Arch Ital Urol Androl. 2009 Dec;81(4):215-7. Arch Ital Urol Androl. 2009. PMID: 20608144
-
Twelve-month prostate-specific antigen values and perineural invasion as strong independent prognostic variables of long-term biochemical outcome after prostate seed brachytherapy.Int J Radiat Oncol Biol Phys. 2012 Nov 15;84(4):962-7. doi: 10.1016/j.ijrobp.2012.01.043. Epub 2012 Apr 9. Int J Radiat Oncol Biol Phys. 2012. PMID: 22494584
-
[I125 low dose rate brachytherapy in localized prostate cancer. Preliminary results after 5 years].Arch Esp Urol. 2005 Apr;58(3):213-26; discussion 224. doi: 10.4321/s0004-06142005000300005. Arch Esp Urol. 2005. PMID: 15906615 Review. Spanish.
Cited by
-
Success of 125I-Seed Treatment in Vulvar Squamous-Cell Carcinoma with Aplastic Anemia: A Case Report.Onco Targets Ther. 2020 Dec 7;13:12561-12566. doi: 10.2147/OTT.S283006. eCollection 2020. Onco Targets Ther. 2020. PMID: 33324074 Free PMC article.
-
Patient assessment of lower urinary tract symptoms using the international prostate symptom score following low-dose-rate prostate brachytherapy.Brachytherapy. 2021 Nov-Dec;20(6):1107-1113. doi: 10.1016/j.brachy.2021.05.009. Epub 2021 Aug 2. Brachytherapy. 2021. PMID: 34353749 Free PMC article.
-
Eligibility criteria according to EAU/ESTRO/SIOG guidelines for exclusive iodine-125 brachytherapy for intermediate-risk prostate adenocarcinoma patients: impact on relapse-free survival.J Contemp Brachytherapy. 2021 Aug;13(4):373-386. doi: 10.5114/jcb.2021.108592. Epub 2021 Aug 24. J Contemp Brachytherapy. 2021. PMID: 34484351 Free PMC article.
-
A Review on Curability of Cancers: More Efforts for Novel Therapeutic Options Are Needed.Cancers (Basel). 2019 Nov 13;11(11):1782. doi: 10.3390/cancers11111782. Cancers (Basel). 2019. PMID: 31766180 Free PMC article. Review.
-
A Case of Iodine 125 Seeds (I-125) Responding to Lung Squamous Cell Carcinoma.Dose Response. 2022 May 19;20(2):15593258221103373. doi: 10.1177/15593258221103373. eCollection 2022 Apr-Jun. Dose Response. 2022. PMID: 35615569 Free PMC article.
References
-
- Roach M, 3rd, Hanks G, Thames H, Jr, Schellhammer P, Shipley WU, Sokol GH, et al. Defining biochemical failure following radiotherapy with or without hormonal therapy in men with clinically localized prostate cancer: recommendations of the RTOG-ASTRO Phoenix Consensus Conference. Int J Radiat Oncol Biol Phys. 2006;65:965–974. - PubMed
-
- Emara AM, Chadwick E, Nobes JP, Abdelbaky AM, Laing RW, Langley SE. Long-term toxicity and quality of life up to 10 years after low-dose rate brachytherapy for prostate cancer. BJU Int. 2012;109:994–1000. Erratum in: BJU Int. 2015;116:E4. - PubMed
-
- Henderson A, Laing RW, Langley SE. Quality of life following treatment for early prostate cancer: does low dose rate (LDR) brachytherapy offer a better outcome? A review. Eur Urol. 2004;45:134–141. - PubMed
-
- Nag S, Beyer D, Friedland J, Grimm P, Nath R. American Brachytherapy Society (ABS) recommendations for transperineal permanent brachytherapy of prostate cancer. Int J Radiat Oncol Biol Phys. 1999;44:789–799. - PubMed
-
- Nath R, Anderson LL, Luxton G, Weaver KA, Williamson JF, Meigooni AS. Dosimetry of interstitial brachytherapy sources: recommendations of the AAPM Radiation Therapy Committee Task Group No. 43. American Association of Physicists in Medicine. Med Phys. 1995;22:209–234. Erratum in: Med Phys 1996;23:1579. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous