

Using a Human Challenge Model of Infection to Measure Vaccine Efficacy: A Randomised, Controlled Trial Comparing the Typhoid Vaccines M01ZH09 with Placebo and Ty21a
- PMID: 27533046
- PMCID: PMC4988630
- DOI: 10.1371/journal.pntd.0004926
Using a Human Challenge Model of Infection to Measure Vaccine Efficacy: A Randomised, Controlled Trial Comparing the Typhoid Vaccines M01ZH09 with Placebo and Ty21a
Abstract
Background: Typhoid persists as a major cause of global morbidity. While several licensed vaccines to prevent typhoid are available, they are of only moderate efficacy and unsuitable for use in children less than two years of age. Development of new efficacious vaccines is complicated by the human host-restriction of Salmonella enterica serovar Typhi (S. Typhi) and lack of clear correlates of protection. In this study, we aimed to evaluate the protective efficacy of a single dose of the oral vaccine candidate, M01ZH09, in susceptible volunteers by direct typhoid challenge.
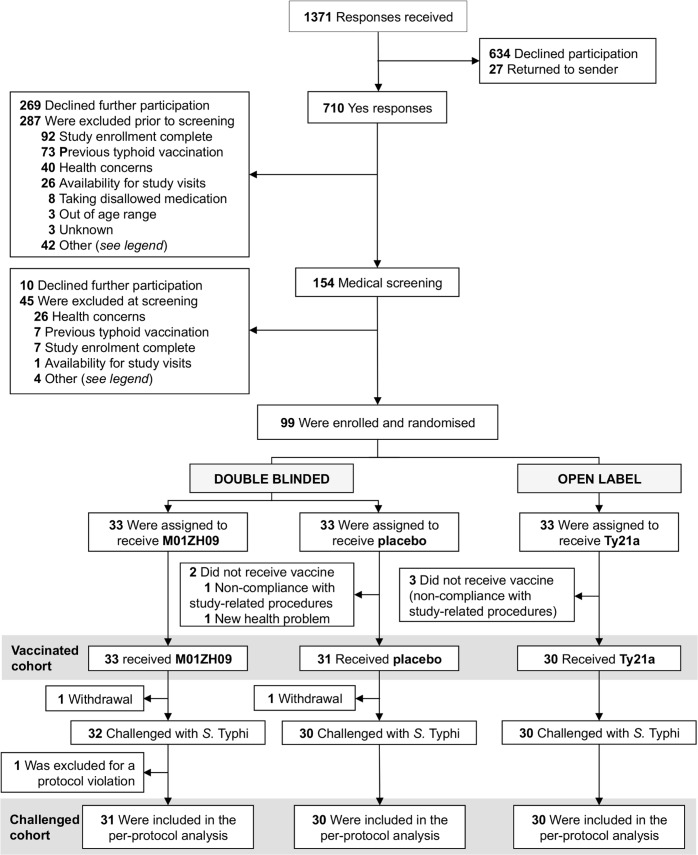
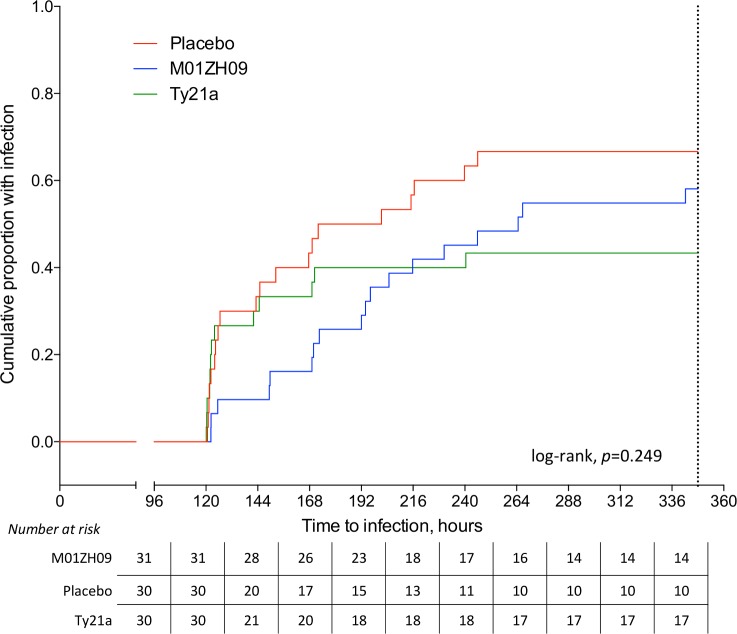
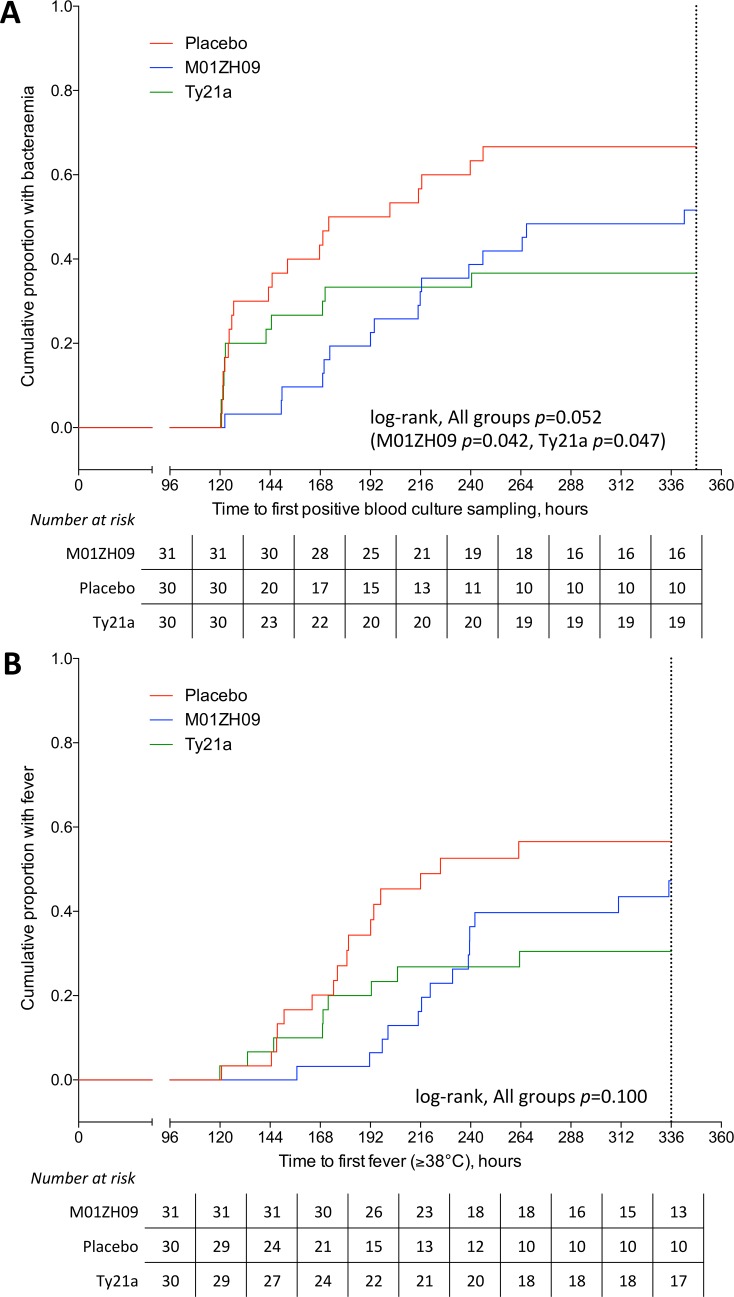
Methods and findings: We performed a randomised, double-blind, placebo-controlled trial in healthy adult participants at a single centre in Oxford (UK). Participants were allocated to receive one dose of double-blinded M01ZH09 or placebo or 3-doses of open-label Ty21a. Twenty-eight days after vaccination, participants were challenged with 104CFU S. Typhi Quailes strain. The efficacy of M01ZH09 compared with placebo (primary outcome) was assessed as the percentage of participants reaching pre-defined endpoints constituting typhoid diagnosis (fever and/or bacteraemia) during the 14 days after challenge. Ninety-nine participants were randomised to receive M01ZH09 (n = 33), placebo (n = 33) or 3-doses of Ty21a (n = 33). After challenge, typhoid was diagnosed in 18/31 (58.1% [95% CI 39.1 to 75.5]) M01ZH09, 20/30 (66.7% [47.2 to 87.2]) placebo, and 13/30 (43.3% [25.5 to 62.6]) Ty21a vaccine recipients. Vaccine efficacy (VE) for one dose of M01ZH09 was 13% [95% CI -29 to 41] and 35% [-5 to 60] for 3-doses of Ty21a. Retrospective multivariable analyses demonstrated that pre-existing anti-Vi antibody significantly reduced susceptibility to infection after challenge; a 1 log increase in anti-Vi IgG resulting in a 71% decrease in the hazard ratio of typhoid diagnosis ([95% CI 30 to 88%], p = 0.006) during the 14 day challenge period. Limitations to the study included the requirement to limit the challenge period prior to treatment to 2 weeks, the intensity of the study procedures and the high challenge dose used resulting in a stringent model.
Conclusions: Despite successfully demonstrating the use of a human challenge study to directly evaluate vaccine efficacy, a single-dose M01ZH09 failed to demonstrate significant protection after challenge with virulent Salmonella Typhi in this model. Anti-Vi antibody detected prior to vaccination played a major role in outcome after challenge.
Trial registration: ClinicalTrials.gov (NCT01405521) and EudraCT (number 2011-000381-35).
Conflict of interest statement
I have read the journal's policy and the authors of this manuscript have the following competing interests: ZH is a named inventor of a patent (US7887816 B2) now owned by Prokarium Ltd, UK. ZH and SL were paid employees of Emergent BioSolutions at the time this trial was performed. All other authors have declared that no competing interests exist.
Figures
References
-
- Lozano R, Naghavi M, Foreman K, Lim S, Shibuya K, Aboyans V, et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380(9859):2095–128. Epub 2012/12/19. 10.1016/S0140-6736(12)61728-0 - DOI - PMC - PubMed
-
- World Health Organisation. Meeting of the Strategic Advisory Group of Experts on Immunization, November 2010—summary, conclusions and recommendations. Weekly Epidemiological Record. 2011;86(1–2):1–16.
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
