

Cholesterol and prostate cancer risk: a long-term prospective cohort study
- PMID: 27535659
- PMCID: PMC4989293
- DOI: 10.1186/s12885-016-2691-5
Cholesterol and prostate cancer risk: a long-term prospective cohort study
Abstract
Background: Few studies have taken risk of competing events into account when examining the relationship between cholesterol and prostate cancer incidence, and few studies have a follow-up over several decades. We aimed to use these approaches to examine the relationship between cholesterol and prostate cancer.
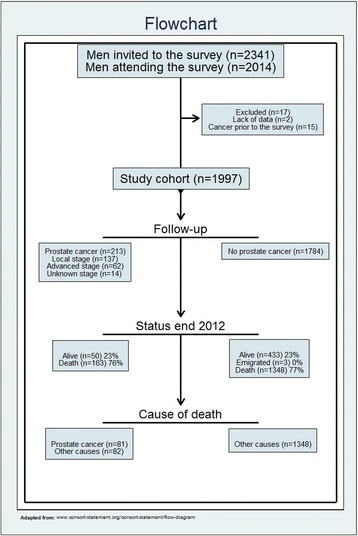
Methods: A cohort of 1997 healthy Norwegian men aged 40-59 years in 1972-75 was followed throughout 2012. Cancer data were extracted from the Cancer Registry of Norway. The association between cholesterol and prostate cancer incidence was assessed using competing risk regression analysis, with adjustment for potential confounders. Date and cause of death was obtained from the Cause of Death Registry of Norway.
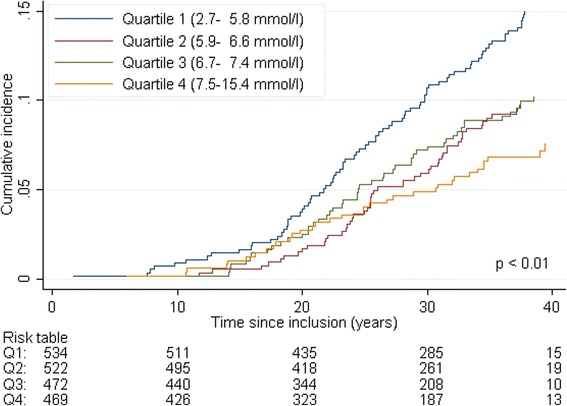
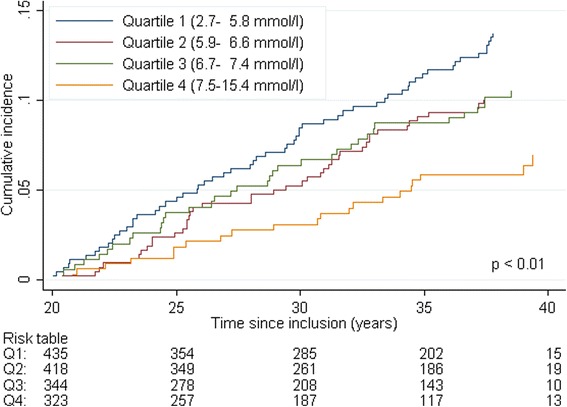
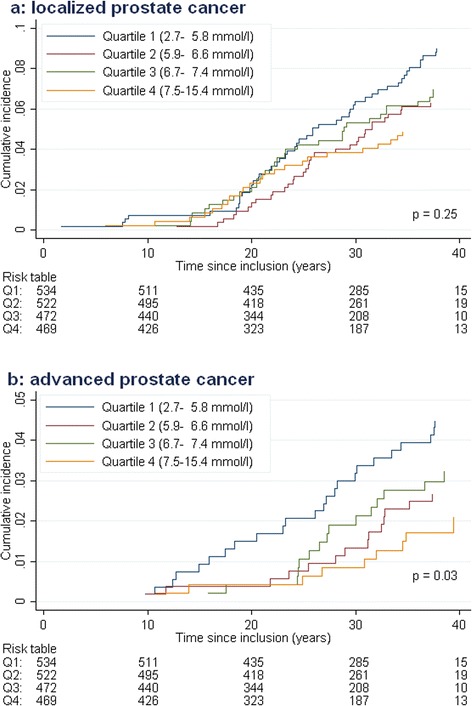
Results: The study cohort had a cancer risk similar to the general Norwegian population. Prostate cancer was registered in 213 men (11 %), including 62 (3 %) with advanced stage at diagnosis. For overall and advanced stage prostate cancer, the incidence was twice as high in the lowest quartile of cholesterol compared to the highest quartile. These associations remained significant after adjustment for age, smoking, physical fitness, BMI, and systolic blood pressure. Furthermore, high physical fitness and low BMI were associated with increased prostate cancer incidence. Sensitivity analyses excluding events during the first 20 years of observation revealed similar results.
Conclusion: Low cholesterol, as well as high physical fitness and low BMI, may be associated with increased risk of prostate cancer. These findings conflict with current prostate cancer prevention recommendations.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
