

Validation of undergraduate medical student script concordance test (SCT) scores on the clinical assessment of the acute abdomen
- PMID: 27535826
- PMCID: PMC4989333
- DOI: 10.1186/s12893-016-0173-y
Validation of undergraduate medical student script concordance test (SCT) scores on the clinical assessment of the acute abdomen
Abstract
Background: Health professionals often manage medical problems in critical situations under time pressure and on the basis of vague information. In recent years, dual process theory has provided a framework of cognitive processes to assist students in developing clinical reasoning skills critical especially in surgery due to the high workload and the elevated stress levels. However, clinical reasoning skills can be observed only indirectly and the corresponding constructs are difficult to measure in order to assess student performance. The script concordance test has been established in this field. A number of studies suggest that the test delivers a valid assessment of clinical reasoning. However, different scoring methods have been suggested. They reflect different interpretations of the underlying construct. In this work we want to shed light on the theoretical framework of script theory and give an idea of script concordance testing. We constructed a script concordance test in the clinical context of "acute abdomen" and compared previously proposed scores with regard to their validity.
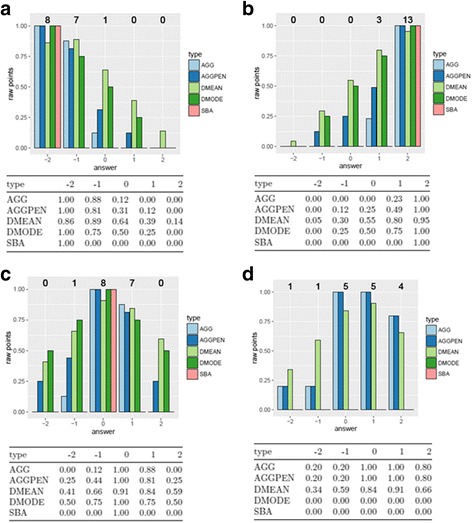
Methods: A test comprising 52 items in 18 clinical scenarios was developed, revised along the guidelines and administered to 56 4(th) and 5(th) year medical students at the end of a blended-learning seminar. We scored the answers using five different scoring methods (distance (2×), aggregate (2×), single best answer) and compared the scoring keys, the resulting final scores and Cronbach's α after normalization of the raw scores.
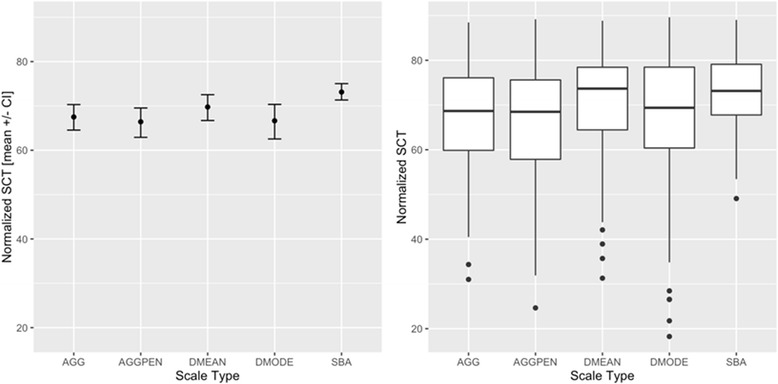
Results: All scores except the single best answers calculation achieved acceptable reliability scores (>= 0.75), as measured by Cronbach's α. Students were clearly distinguishable from the experts, whose results were set to a mean of 80 and SD of 5 by the normalization process. With the two aggregate scoring methods, the students' means values were between 62.5 (AGGPEN) and 63.9 (AGG) equivalent to about three expert SD below the experts' mean value (Cronbach's α : 0.76 (AGGPEN) and 0.75 (AGG)). With the two distance scoring methods the students' mean was between 62.8 (DMODE) and 66.8 (DMEAN) equivalent to about two expert SD below the experts' mean value (Cronbach's α: 0.77 (DMODE) and 0.79 (DMEAN)). In this study the single best answer (SBA) scoring key yielded the worst psychometric results (Cronbach's α: 0.68).
Conclusion: Assuming the psychometric properties of the script concordance test scores are valid, then clinical reasoning skills can be measured reliably with different scoring keys in the SCT presented here. Psychometrically, the distance methods seem to be superior, wherein inherent statistical properties of the scales might play a significant role. For methodological reasons, the aggregate methods can also be used. Despite the limitations and complexity of the underlying scoring process and the calculation of reliability, we advocate for SCT because it allows a new perspective on the measurement and teaching of cognitive skills.
Keywords: Acute abdomen; Assessment; Clinical reasoning; Medical education; Scales; Script concordance test; Surgery.
Figures
Similar articles
-
Can script concordance testing be used in nursing education to accurately assess clinical reasoning skills?J Nurs Educ. 2014 May 1;53(5):281-6. doi: 10.3928/01484834-20140321-03. Epub 2014 Mar 21. J Nurs Educ. 2014. PMID: 24641082
-
Reliability and validity of the script concordance test for postgraduate students of general practice.Eur J Gen Pract. 2017 Dec;23(1):208-213. doi: 10.1080/13814788.2017.1358709. Eur J Gen Pract. 2017. PMID: 28819998 Free PMC article.
-
The psychometric properties of five scoring methods applied to the script concordance test.Acad Med. 2005 Apr;80(4):395-9. doi: 10.1097/00001888-200504000-00019. Acad Med. 2005. PMID: 15793026 Clinical Trial.
-
Threats to validity in the use and interpretation of script concordance test scores.Med Educ. 2013 Dec;47(12):1175-83. doi: 10.1111/medu.12283. Med Educ. 2013. PMID: 24206151 Review.
-
[The Script Concordance Test: A multimodal teaching tool].Rev Med Interne. 2018 Jul;39(7):566-573. doi: 10.1016/j.revmed.2017.12.011. Epub 2018 Mar 22. Rev Med Interne. 2018. PMID: 29576195 Review. French.
Cited by
-
Combination of different clinical reasoning tests in a national exam.J Adv Med Educ Prof. 2019 Oct;7(4):230-234. doi: 10.30476/jamp.2019.83101.1083. J Adv Med Educ Prof. 2019. PMID: 31750362 Free PMC article.
-
Virtual patients in the acquisition of clinical reasoning skills: does presentation mode matter? A quasi-randomized controlled trial.BMC Med Educ. 2017 Sep 15;17(1):165. doi: 10.1186/s12909-017-1004-2. BMC Med Educ. 2017. PMID: 28915871 Free PMC article. Clinical Trial.
-
The Impact of Script Concordance Testing on Clinical Decision-Making in Paramedic Education.Healthcare (Basel). 2024 Jan 22;12(2):282. doi: 10.3390/healthcare12020282. Healthcare (Basel). 2024. PMID: 38275562 Free PMC article.
-
Teaching emergency situations during a psychiatry residency programme using a blended learning approach: a pilot study.BMC Med Educ. 2021 Sep 6;21(1):473. doi: 10.1186/s12909-021-02887-2. BMC Med Educ. 2021. PMID: 34488745 Free PMC article.
-
Development and psychometrics of script concordance test (SCT) in midwifery.Med J Islam Repub Iran. 2018 Aug 23;32:75. doi: 10.14196/mjiri.32.75. eCollection 2018. Med J Islam Repub Iran. 2018. PMID: 30643750 Free PMC article.
References
-
- WFME . World federation for medical education: global standards for quality improvement - the 2015 revision. Copenhagen (Denmark): Ferney-Voltaire (France); 2015.
-
- MFT . National competence based catalogue of learning objectives in medicine (NKLM). [Nationaler Kompetenzbasierter Lernzielkatalog Medizin (NKLM)] 2015.
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
