

PD-1 Inhibitor-Related Pneumonitis in Advanced Cancer Patients: Radiographic Patterns and Clinical Course
- PMID: 27535979
- PMCID: PMC5161686
- DOI: 10.1158/1078-0432.CCR-16-1320
PD-1 Inhibitor-Related Pneumonitis in Advanced Cancer Patients: Radiographic Patterns and Clinical Course
Abstract
Purpose: Investigate the clinical characteristics, radiographic patterns, and treatment course of PD-1 inhibitor-related pneumonitis in advanced cancer patients.
Experimental design: Among patients with advanced melanoma, lung cancer, or lymphoma treated in trials of nivolumab, we identified those who developed pneumonitis. Chest CT scans were reviewed to assess extent, distribution, and radiographic patterns of pneumonitis.
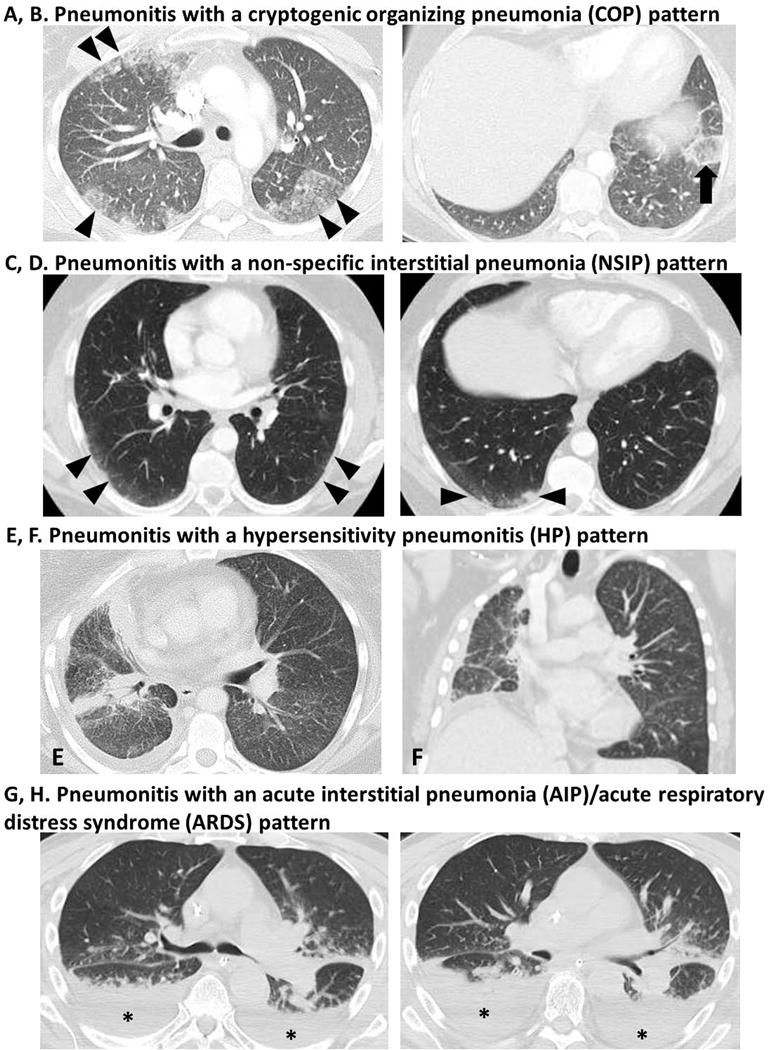
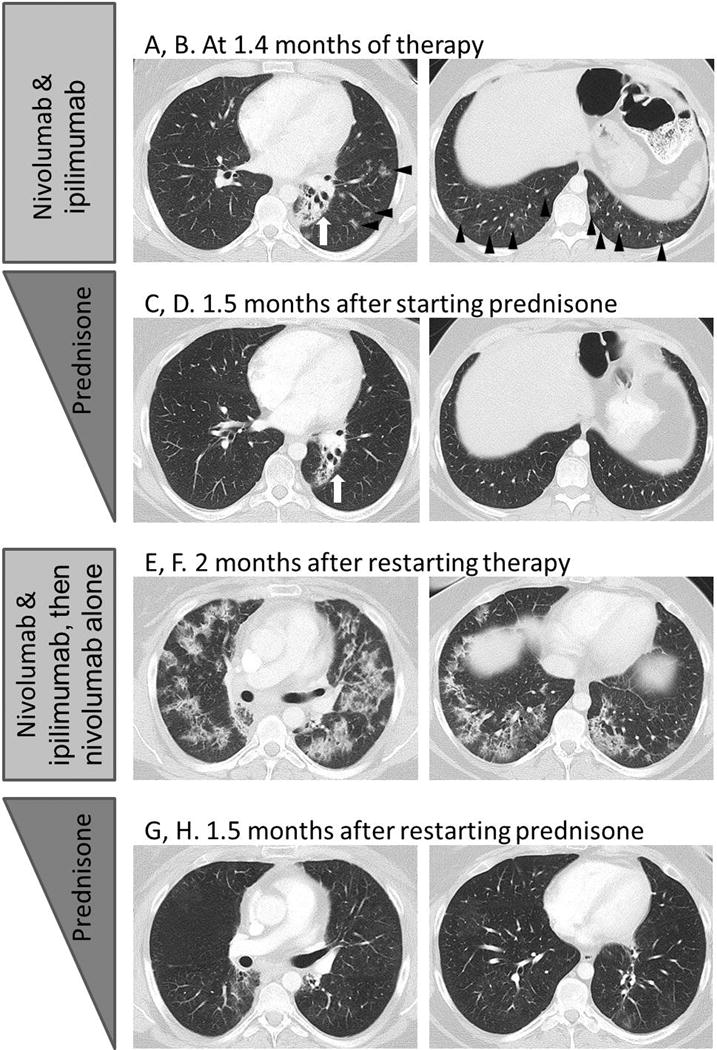
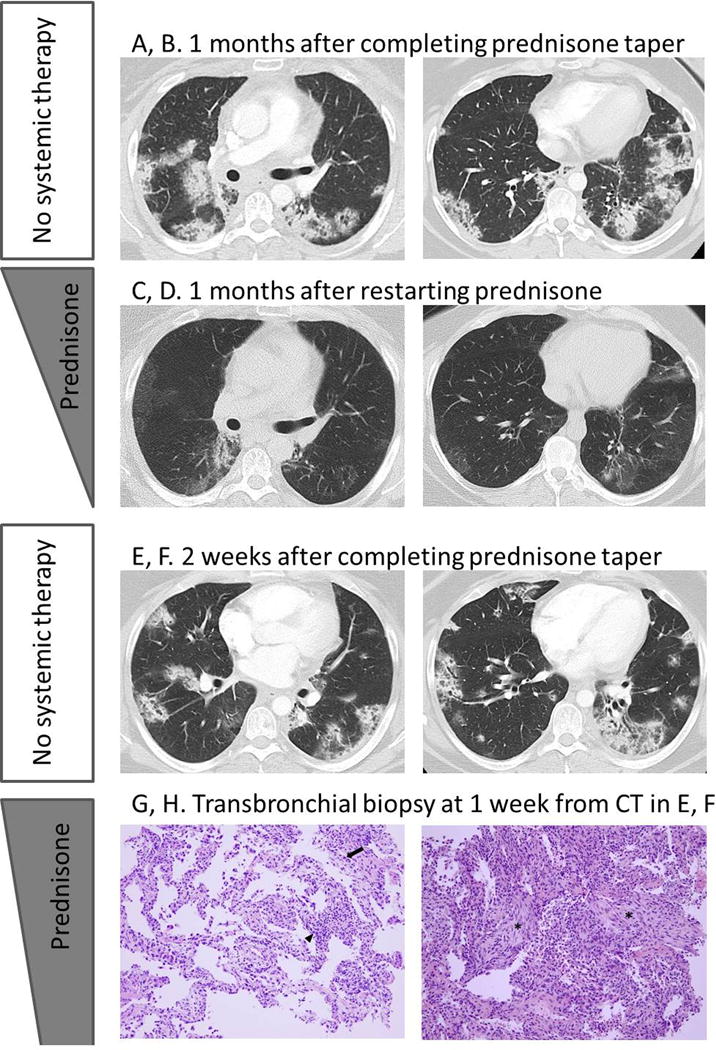
Results: Among 170 patients treated in 10 different trials of nivolumab, 20 patients (10 melanoma, 6 lymphoma, and 4 lung cancer) developed pneumonitis. Five patients received nivolumab monotherapy, and 15 received combination therapy. The median time from therapy initiation to pneumonitis was 2.6 months. Radiographic pattern was cryptogenic organizing pneumonia (COP) in 13, nonspecific interstitial pneumonia (NSIP) in 3, hypersensitivity pneumonitis (HP) in 2, and acute interstitial pneumonia (AIP)/acute respiratory distress syndrome (ARDS) in 2 patients. The AIP/ARDS pattern had the highest grade, followed by COP, whereas NSIP and HP had lower grade (median grade: 3, 2, 1, 1, respectively; P = 0.006). The COP pattern was most common in all tumors and treatment regimens. Most patients (17/20; 85%) received corticosteroids, and 3 (15%) also required infliximab. Seven patients restarted nivolumab therapy; 2 of them developed recurrent pneumonitis and were successfully retreated with corticosteroids. One of the patients experienced a pneumonitis flare after completion of corticosteroid taper without nivolumab retreatment.
Conclusions: PD-1 inhibitor-related pneumonitis showed a spectrum of radiographic patterns, reflecting pneumonitis grades. COP was the most common pattern across tumor types and therapeutic regimens. Most patients were successfully treated with corticosteroids. Recurrent pneumonitis and pneumonitis flare were noted in a few patients. Clin Cancer Res; 22(24); 6051-60. ©2016 AACRSee related commentary by Castanon, p. 5956.
©2016 American Association for Cancer Research.
Conflict of interest statement
Nishino: Consultant to Bristol-Myers Squibb, Toshiba Medical Systems, WorldCare Clinical; Research grant from Merck Investigator Studies Program. Ramaiya: Nothing to disclose Awad: Consultant to AstraZeneca, AbbVie, Boehringer-Ingelheim, Merck, Pfizer, Genentech. Research grant from the Conquer Cancer Foundation of the American Society of Clinical Oncology; and the International Association for the Study of Lung Cancer Sholl: Scientific advisory board for Genentech Maattala: Nothing to disclose Taibi: Nothing to disclose Hatabu: Research support from Canon Inc, Toshiba Medical systems, AZE Inc., Konica-Minolta inc.; Consultant to Toshiba Medical systems Ott: Dr. Ott has served as a consultant to Bristol-Myers Squibb and has received clinical trial support from Bristol-Myers Squibb and Merck. Armand: Dr. Armand has served as a consultant to Bristol-Myers Squibb, Merck, and Infinity Pharmaceuticals, and has received clinical trial support from Bristol-Myers Squibb, Merck, Tensha Therapeutics, Sequenta, Otsuka, and Sigma-Tau. Hodi: Dr. Hodi has served as a non-paid consultant to Bristol-Myers Squibb and has received clinical trial support from Bristol-Myers Squibb, advisor and clinical trial support from Merck, and advisor and clinical trial support from Genentech, consultant to Novartis and Amgen.
Figures
Similar articles
-
Anti-PD-1 Inhibitor-Related Pneumonitis in Non-Small Cell Lung Cancer.Cancer Immunol Res. 2016 Apr;4(4):289-93. doi: 10.1158/2326-6066.CIR-15-0267. Epub 2016 Feb 10. Cancer Immunol Res. 2016. PMID: 26865455 Free PMC article.
-
Drug-related pneumonitis during mammalian target of rapamycin inhibitor therapy in patients with neuroendocrine tumors: a radiographic pattern-based approach.Eur J Cancer. 2016 Jan;53:163-70. doi: 10.1016/j.ejca.2015.10.015. Epub 2016 Jan 4. Eur J Cancer. 2016. PMID: 26760924 Free PMC article.
-
Drug-Related Pneumonitis During Mammalian Target of Rapamycin Inhibitor Therapy: Radiographic Pattern-Based Approach in Waldenström Macroglobulinemia as a Paradigm.Oncologist. 2015 Sep;20(9):1077-83. doi: 10.1634/theoncologist.2015-0033. Epub 2015 Jul 23. Oncologist. 2015. PMID: 26205737 Free PMC article.
-
High incidence and early onset of nivolumab-induced pneumonitis: four case reports and literature review.BMC Pulm Med. 2018 Jan 30;18(1):23. doi: 10.1186/s12890-018-0592-x. BMC Pulm Med. 2018. PMID: 29378571 Free PMC article. Review.
-
[Immune-related pneumonitis caused by programmed death-1 inhibitor Pembrolizumab: a case report and literature review].Zhonghua Jie He He Hu Xi Za Zhi. 2017 Oct 12;40(10):736-743. doi: 10.3760/cma.j.issn.1001-0939.2017.10.006. Zhonghua Jie He He Hu Xi Za Zhi. 2017. PMID: 29050127 Review. Chinese.
Cited by
-
Clinical implications of bronchoscopy for immune checkpoint inhibitor-related pneumonitis in patients with non-small cell lung cancer.BMC Pulm Med. 2021 May 8;21(1):155. doi: 10.1186/s12890-021-01523-5. BMC Pulm Med. 2021. PMID: 33964920 Free PMC article.
-
Immune Checkpoint Inhibitor-Associated Pneumonitis in Non-Small Cell Lung Cancer: Current Understanding in Characteristics, Diagnosis, and Management.Front Immunol. 2021 May 28;12:663986. doi: 10.3389/fimmu.2021.663986. eCollection 2021. Front Immunol. 2021. PMID: 34122422 Free PMC article. Review.
-
Rate and risk factors of recurrent immune checkpoint inhibitor-related pneumonitis in patients with lung cancer.Transl Lung Cancer Res. 2022 Mar;11(3):381-392. doi: 10.21037/tlcr-22-168. Transl Lung Cancer Res. 2022. PMID: 35399572 Free PMC article.
-
Nintedanib allows retreatment with atezolizumab of combined non-small cell lung cancer/idiopathic pulmonary fibrosis after atezolizumab-induced pneumonitis: a case report.BMC Pulm Med. 2019 Aug 22;19(1):156. doi: 10.1186/s12890-019-0920-9. BMC Pulm Med. 2019. PMID: 31438923 Free PMC article.
-
Imaging features of toxicities associated with immune checkpoint inhibitors.Eur J Radiol Open. 2022 Aug 8;9:100434. doi: 10.1016/j.ejro.2022.100434. eCollection 2022. Eur J Radiol Open. 2022. PMID: 35967881 Free PMC article.
References
-
- Robert C, Ribas A, Wolchok JD, et al. Anti-programmed-death-receptor-1 treatment with pembrolizumab in ipilimumab-refractory advanced melanoma: a randomised dose-comparison cohort of a phase 1 trial. Lancet. 2014;384:1109–1117. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
