

Randomized placebo-controlled study of intravenous methylnaltrexone in postoperative ileus
- PMID: 27536446
- PMCID: PMC4937649
- DOI: 10.3109/21556660.2013.838169
Randomized placebo-controlled study of intravenous methylnaltrexone in postoperative ileus
Abstract
Objective: This phase 2 study evaluated the safety and activity of intravenous methylnaltrexone on the duration of postoperative ileus in patients undergoing segmental colectomy.
Methods: Adults (aged 18 years or older) with American Society of Anesthesiologists physical status of I, II, or III who underwent segmental colectomy, including partial colectomy, sigmoidectomy, cecectomy, or anterior proctosigmoidectomy, via laparotomy with general anesthesia, received intravenous methylnaltrexone 0.30 mg/kg or placebo every 6 h beginning within 90 min after end of surgery. Treatment continued until 24 h after the patient tolerated solid foods, was discharged, or for 7 d maximum. Efficacy endpoints included measures of gastrointestinal recovery and time to discharge eligibility.
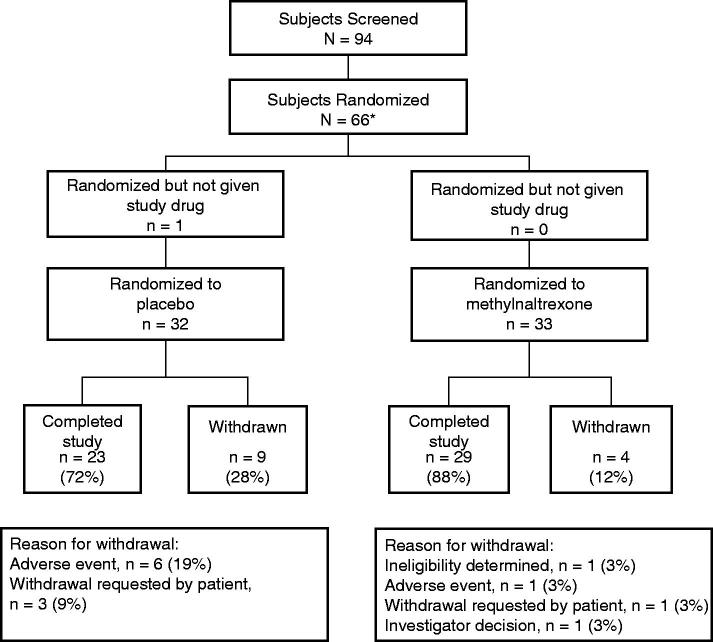
Results: A total of 65 patients (methylnaltrexone, n = 33; placebo, n = 32) were randomized. Mean time to first bowel movement was accelerated by 20 h (p = 0.038) and time to discharge eligibility was accelerated by 33 h (p = 0.049) with methylnaltrexone vs placebo. Opioid use was similar between groups until postoperative day 4, then fluctuated in the placebo group. Methylnaltrexone was generally well tolerated.
Conclusions: In this study, intravenous methylnaltrexone significantly decreased time to postoperative bowel recovery and eligibility for hospital discharge by ∼1 d, with an adverse event profile similar to placebo. These were two of several exploratory endpoints; not all efficacy endpoints showed a significant difference between methylnaltrexone and placebo. The efficacy results in this trial were not seen in two subsequent large-scale studies.
Keywords: Methylnaltrexone; Mu-opioid receptor antagonist; Opioids; Postoperative ileus.
Figures
Similar articles
-
Safety and efficacy of methylnaltrexone in shortening the duration of postoperative ileus following segmental colectomy: results of two randomized, placebo-controlled phase 3 trials.Dis Colon Rectum. 2011 May;54(5):570-8. doi: 10.1007/DCR.0b013e3182092bde. Dis Colon Rectum. 2011. PMID: 21471758 Clinical Trial.
-
Perioperative subcutaneous methylnaltrexone does not enhance gastrointestinal recovery after posterior short-segment spinal arthrodesis surgery: a randomized controlled trial.Spine J. 2022 Mar;22(3):444-453. doi: 10.1016/j.spinee.2021.08.004. Epub 2021 Aug 19. Spine J. 2022. PMID: 34419626 Clinical Trial.
-
Alvimopan, a novel, peripherally acting mu opioid antagonist: results of a multicenter, randomized, double-blind, placebo-controlled, phase III trial of major abdominal surgery and postoperative ileus.Ann Surg. 2004 Oct;240(4):728-34; discussion 734-5. doi: 10.1097/01.sla.0000141158.27977.66. Ann Surg. 2004. PMID: 15383800 Free PMC article. Clinical Trial.
-
Methylnaltrexone: MNTX.Drugs R D. 2006;7(6):374-8. doi: 10.2165/00126839-200607060-00006. Drugs R D. 2006. PMID: 17073520 Review.
-
Mitoxantrone: a review of its use in multiple sclerosis.CNS Drugs. 2004;18(6):379-96. doi: 10.2165/00023210-200418060-00010. CNS Drugs. 2004. PMID: 15089110 Review.
Cited by
-
Global cost of postoperative ileus following abdominal surgery: meta-analysis.BJS Open. 2023 May 5;7(3):zrad054. doi: 10.1093/bjsopen/zrad054. BJS Open. 2023. PMID: 37352872 Free PMC article.
-
Selective Opioid Antagonists Following Bowel Resection for Prevention of Postoperative Ileus: a Systematic Review and Meta-analysis.J Gastrointest Surg. 2021 Jun;25(6):1601-1624. doi: 10.1007/s11605-021-04973-8. Epub 2021 Mar 25. J Gastrointest Surg. 2021. PMID: 33768428
-
Peripherally Acting μ-Opioid Receptor Antagonists in the Management of Postoperative Ileus: a Clinical Review.J Gastrointest Surg. 2021 Jan;25(1):293-302. doi: 10.1007/s11605-020-04671-x. Epub 2020 Aug 10. J Gastrointest Surg. 2021. PMID: 32779081 Free PMC article. Review.
-
State-of-the-art colorectal disease: postoperative ileus.Int J Colorectal Dis. 2021 Sep;36(9):2017-2025. doi: 10.1007/s00384-021-03939-1. Epub 2021 May 11. Int J Colorectal Dis. 2021. PMID: 33977334 Free PMC article. Review.
-
Methylnaltrexone's Effect on Cholestasis in Trauma Patients.Cureus. 2024 Sep 19;16(9):e69750. doi: 10.7759/cureus.69750. eCollection 2024 Sep. Cureus. 2024. PMID: 39429257 Free PMC article.
References
-
- Kehlet H, Holte K. Review of postoperative ileus. Am J Surg 2001;182(5A Suppl):3S–10S - PubMed
-
- Taguchi A Sharma N Saleem RM et al. Selective postoperative inhibition of gastrointestinal opioid receptors. N Engl J Med 2001;345:935–40 - PubMed
-
- Brix-Christensen V Tonnesen E Sanchez RG et al. Endogenous morphine levels increase following cardiac surgery as part of the antiinflammatory response? Int J Cardiol 1997;62:191–7 - PubMed
-
- Yoshida S Ohta J Yamasaki K et al. Effect of surgical stress on endogenous morphine and cytokine levels in the plasma after laparoscopic or open cholecystectomy. Surg Endosc 2000;14:137–40 - PubMed
-
- Sanger GJ, Tuladhar BR. The role of endogenous opioids in the control of gastrointestinal motility: predictions from in vitro modelling. Neurogastroenterol Motil 2004;16(Suppl 2):38–45 - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials