

Low-cost Design and Manufacturing of Surgical Guides for Mandibular Reconstruction Using a Fibula
- PMID: 27536484
- PMCID: PMC4977133
- DOI: 10.1097/GOX.0000000000000682
Low-cost Design and Manufacturing of Surgical Guides for Mandibular Reconstruction Using a Fibula
Abstract
Background: Surgical cutting guides are used in mandibular reconstruction involving osteotomy of the mandible and fibula. Cutting guides produced using computer-aided design (CAD) and computer-aided manufacturing (CAM) technologies have been reported recently. These guides aim to increase the benefits to patients by improving the accuracy, shortening the operating time, and correcting occlusion. However, the availability of these advanced technologies is limited in some regions of the world. To test whether we could produce low-cost surgical cutting guides, we made surgical guides and investigated their accuracy.
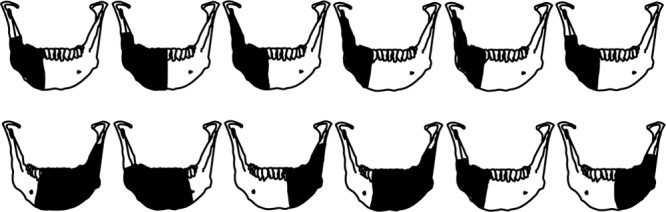
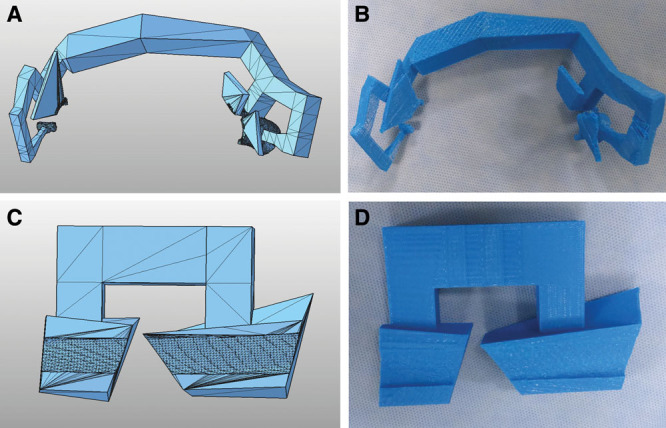
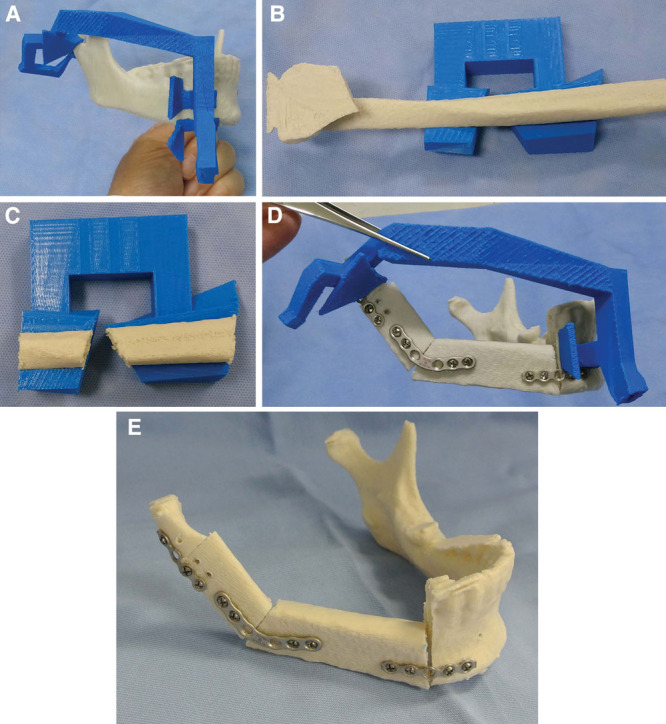
Methods: Using free CAD software, we designed surgical cutting guides for the mandible and fibula and used these to perform virtual mandibular segmental osteotomies and fibula transplants in 12 model surgeries. The cutting guides were printed on a 3-dimensional (3D) printer. The model surgeries were performed using 3D mandibular models and cutting guides to check their accuracy. Deviations between the virtually simulated plan and the actual model surgery were investigated.
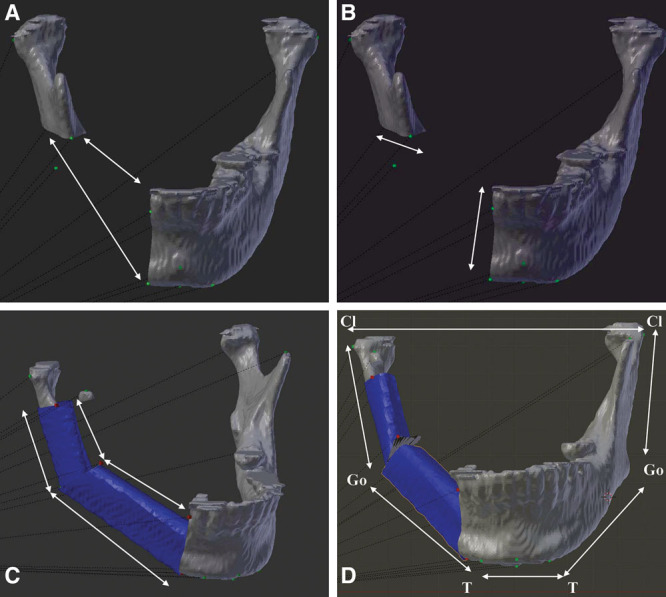
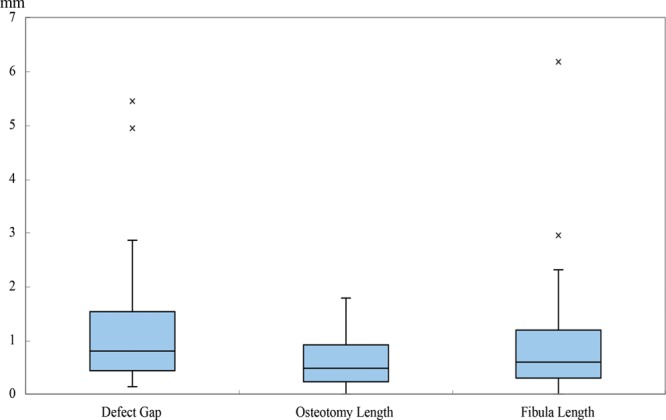
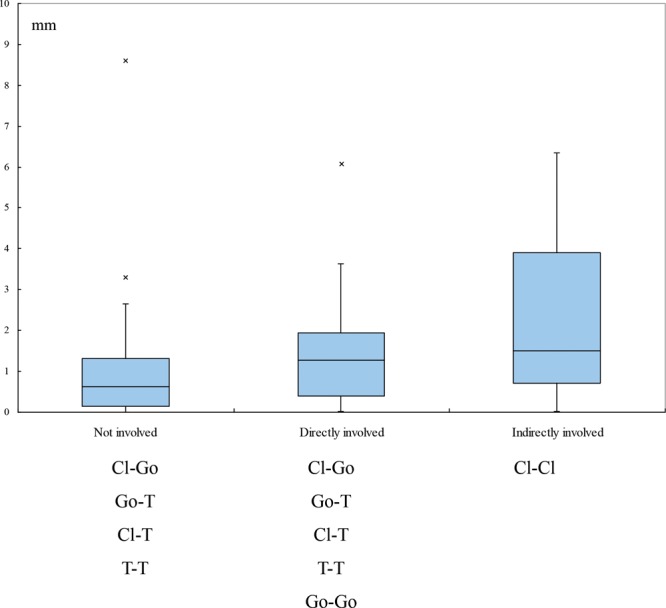
Results: CAD and CAM technologies were used to design and 3D print the cutting guides and models. The guided surgeries were performed. The deviations were about 1.3 mm for mandibular osteotomy, less than 1 mm for fibular osteotomy, and within 2.4 mm for reconstructions of the mandible.
Conclusions: Without using expensive software or products, we were able to design surgical cutting guides for the mandible and fibula and used these to perform virtual simulation of mandibular segmental osteotomy and fibular reconstruction. Model surgeries using 3D-printed surgical guides showed that the accuracy of reconstruction was within a 3-mm deviation. In circumstances where commercial CAD/CAM guides are not available, it may be possible to use CAD/CAM surgical guides in the clinic if doctors are willing to volunteer their time for the design and printing.
Figures
Similar articles
-
[How to make your own custom cutting guides for both mandibular and fibular stair step osteotomies?].Ann Chir Plast Esthet. 2017 Dec;62(6):652-658. doi: 10.1016/j.anplas.2017.03.005. Epub 2017 Apr 26. Ann Chir Plast Esthet. 2017. PMID: 28456427 French.
-
The Shape of Things to Come: In-Hospital Three-Dimensional Printing for Mandibular Reconstruction Using Fibula Free Flap.Laryngoscope. 2020 Dec;130(12):E811-E816. doi: 10.1002/lary.28650. Epub 2020 Apr 6. Laryngoscope. 2020. PMID: 32249936
-
Does an In-House Computer-Aided Design/Computer-Aided Manufacturing Approach Contribute to Accuracy and Time Shortening in Mandibular Reconstruction?J Craniofac Surg. 2020 Oct;31(7):1928-1932. doi: 10.1097/SCS.0000000000006699. J Craniofac Surg. 2020. PMID: 32649531
-
Computer-Assisted Mandibular Reconstruction using a Patient-Specific Reconstruction Plate Fabricated with Computer-Aided Design and Manufacturing Techniques.Craniomaxillofac Trauma Reconstr. 2014 Jun;7(2):158-66. doi: 10.1055/s-0034-1371356. Epub 2014 Feb 25. Craniomaxillofac Trauma Reconstr. 2014. PMID: 25045420 Free PMC article. Review.
-
Black Bone MRI for Virtual Surgical Planning in Craniomaxillofacial Surgery.Semin Plast Surg. 2022 Dec 7;36(3):192-198. doi: 10.1055/s-0042-1756451. eCollection 2022 Aug. Semin Plast Surg. 2022. PMID: 36506277 Free PMC article. Review.
Cited by
-
Challenges of Integrating New Technologies for Orthopedic Doctors to Face up to Difficulties during the Pandemic Era.Healthcare (Basel). 2023 May 23;11(11):1524. doi: 10.3390/healthcare11111524. Healthcare (Basel). 2023. PMID: 37297666 Free PMC article.
-
In-House Manufacturing of a Translucent Three-Dimensional Model and Surgical Guide for Marginal Mandibulectomy.Cureus. 2024 Feb 23;16(2):e54771. doi: 10.7759/cureus.54771. eCollection 2024 Feb. Cureus. 2024. PMID: 38523915 Free PMC article.
-
Three-Dimensional Printing in Orthopedics: from the Basics to Surgical Applications.Curr Rev Musculoskelet Med. 2021 Feb;14(1):1-8. doi: 10.1007/s12178-020-09691-3. Curr Rev Musculoskelet Med. 2021. PMID: 33409834 Free PMC article. Review.
-
Realizing in-house algorithm-driven free fibula flap set up within 24 hours: a pilot study evaluating accuracy with open-source tools.Front Surg. 2023 Dec 15;10:1321217. doi: 10.3389/fsurg.2023.1321217. eCollection 2023. Front Surg. 2023. PMID: 38162091 Free PMC article.
-
Cost Analysis for In-house versus Industry-printed Skull Models for Acute Midfacial Fractures.Plast Reconstr Surg Glob Open. 2020 May 26;8(5):e2831. doi: 10.1097/GOX.0000000000002831. eCollection 2020 May. Plast Reconstr Surg Glob Open. 2020. PMID: 33154873 Free PMC article.
References
-
- Tarsitano A, Del Corso G, Ciocca L, et al. Mandibular reconstructions using computer-aided design/computer-aided manufacturing: a systematic review of a defect-based reconstructive algorithm. J Craniomaxillofac Surg. 2015;43:1785–1791. - PubMed
-
- Hanasono MM, Skoracki RJ. Computer-assisted design and rapid prototype modeling in microvascular mandible reconstruction. Laryngoscope. 2013;123:597–604. - PubMed
-
- Hirsch DL, Garfein ES, Christensen AM, et al. Use of computer-aided design and computer-aided manufacturing to produce orthognathically ideal surgical outcomes: a paradigm shift in head and neck reconstruction. J Oral Maxillofac Surg. 2009;67:2115–2122. - PubMed
-
- Wilde F, Hanken H, Probst F, et al. Multicenter study on the use of patient-specific CAD/CAM reconstruction plates for mandibular reconstruction. Int J Comput Assist Radiol Surg. 2015;10:2035–2051. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous