

Hemodialysis in Asia
- PMID: 27536677
- PMCID: PMC4934815
- DOI: 10.1159/000441816
Hemodialysis in Asia
Abstract
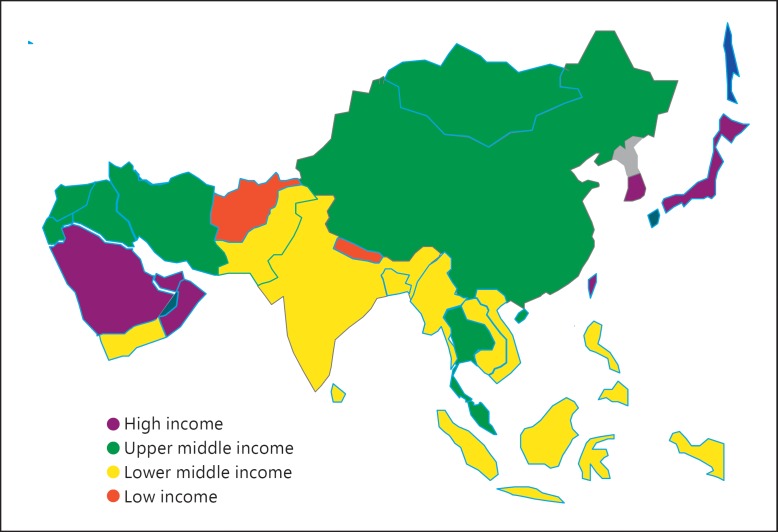
Background: Asia is the largest, most populous and most heterogeneous continent in the world. The number of patients with end-stage renal disease is growing rapidly in Asia.
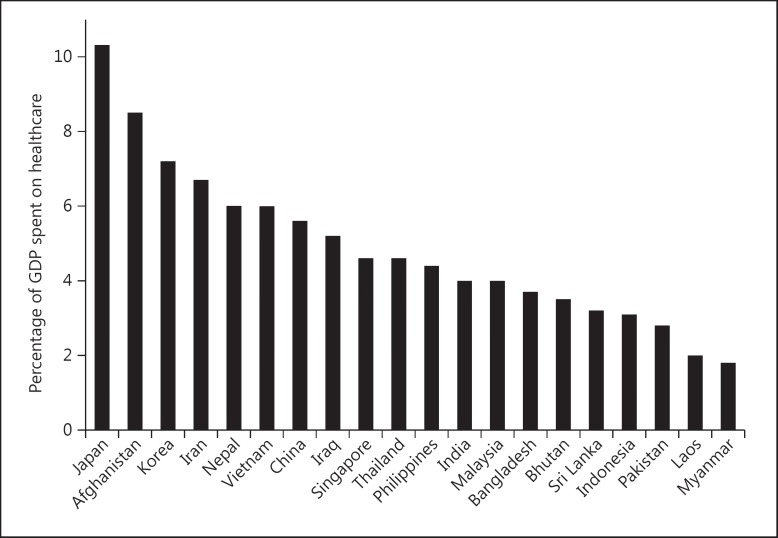
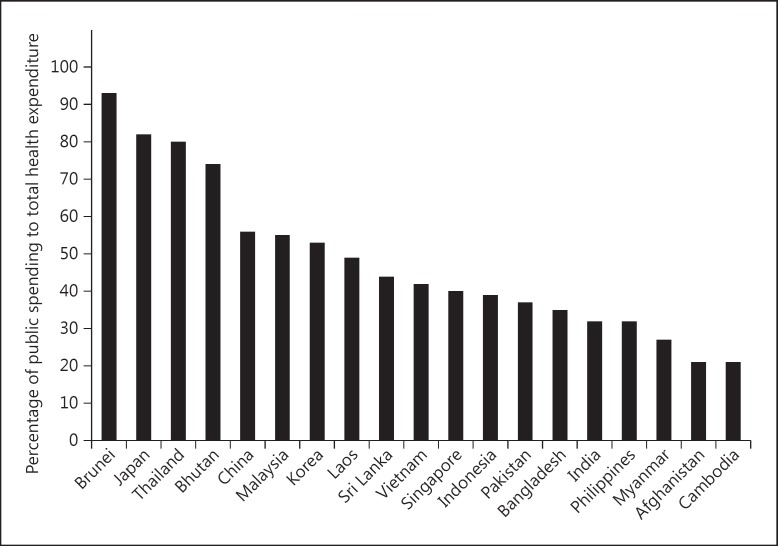
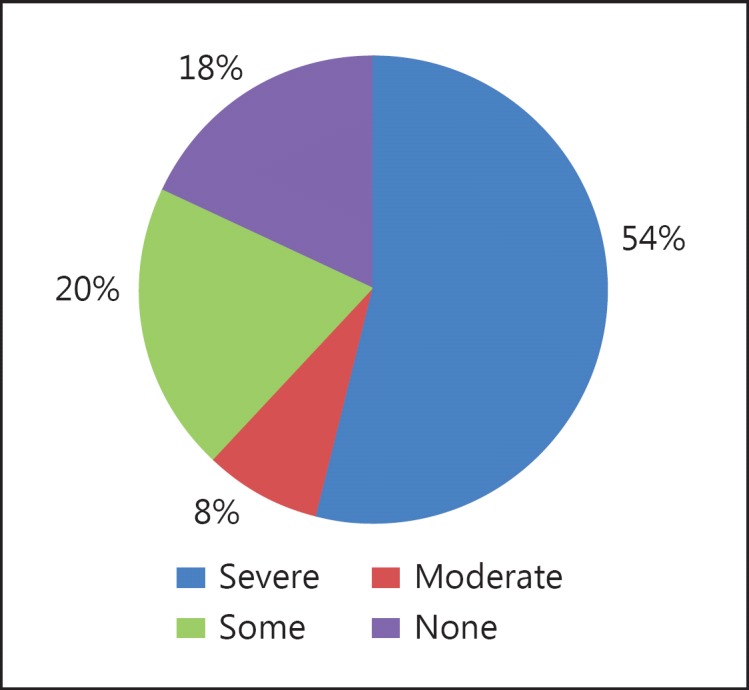
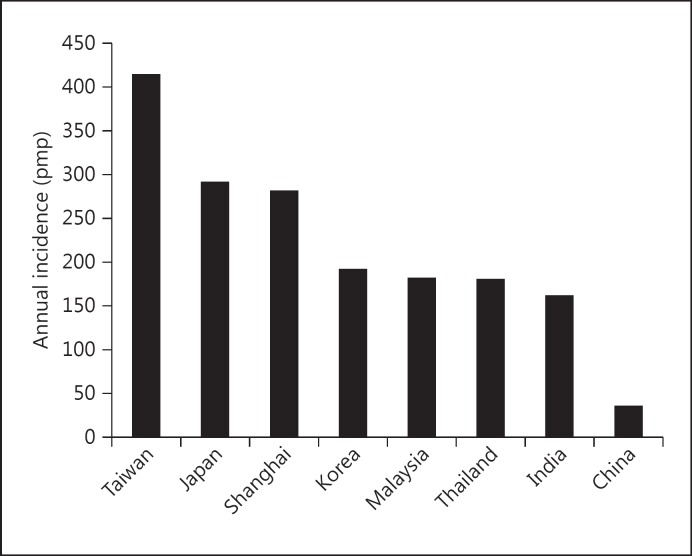
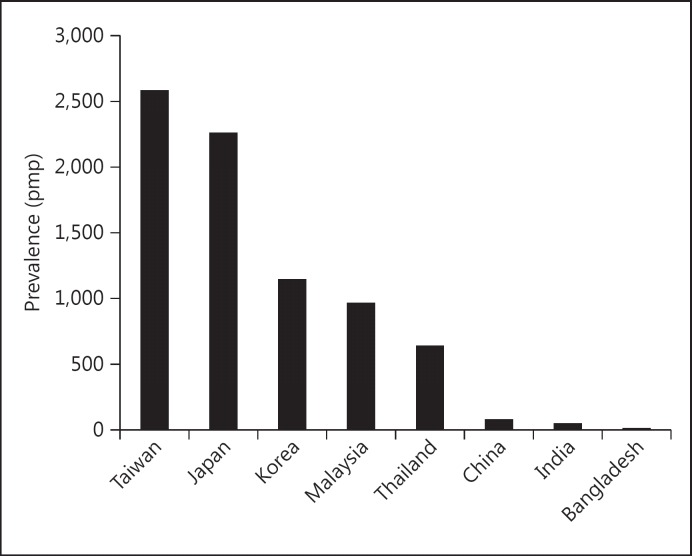
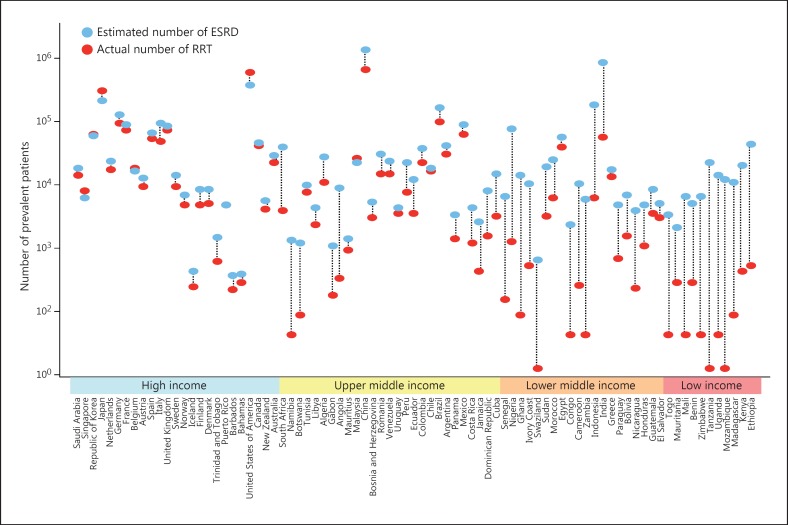
Summary: A fully informed report on the status of dialysis therapies including hemodialysis (HD) is limited by the lack of systematic registries. Available data suggest remarkable heterogeneities, with some countries like Taiwan, Japan and Korea exhibiting well-established HD systems, high prevalence and universal access to all patients, while low- and low-middle income countries are unable to provide HD to eligible patients because of high cost and poor healthcare systems. Many Asian countries have unregulated dialysis units, with poor standards of delivery, quality control and outcome reporting. This leads to high mortality due to preventable complications like infections. Modeling data suggest that at least 2.9 million people need dialysis in Asia, which represents a gap in availability of dialysis to the tune of -66%. The population is projected to grow rapidly in the coming years. Several countries are expanding access to HD. Innovative modifications in dialysis practice are being made to optimize outcomes. It is important to develop robust systems of documentation and outcome reporting to evaluate the effects of such changes. HD needs to develop in conjunction with effective preventive programs and improvement of health systems.
Key messages: The practice of HD in Asia is growing and evolving. Rapid expansion will improve the currently dismal access to care for large sections of the population. Quality issues need to be addressed if the full benefit of this therapy is to reach the population. Developed countries of Asia can provide substantial messages to developing economies. HD programs must develop in conjunction with prevention efforts.
Facts from east and west: (1) While developed Western and Asian countries provide end-stage renal disease patients full access to HD, healthcare systems from South and South-East Asia can offer access to HD only to a limited fraction of the patients in need. Even though the annual costs of HD are much lower in less developed countries (for instance 30 times lower in India compared to the US), patients often cannot afford costs not covered by health insurance. (2) The recommended dialysis pattern in the West is at least three sessions weekly with high-flux dialyzers. Studies from Shanghai and Taiwan might however indicate a benefit of twice versus thrice weekly sessions. In less developed Asian countries, a twice weekly pattern is common, sometimes with dialyzer reuse and inadequate water treatment. A majority of patients decrease session frequency or discontinue the program due to financial constraint. (3) As convective therapies are gaining popularity in Europe, penetration in Asia is low and limited by costs. (4) In Asian countries, in particular in the South and South-East, hepatitis and tuberculosis infections in HD patients are higher than in the West and substantially increase mortality. (5) Progress has recently been made in countries like Thailand and Brunei to provide universal HD access to all patients in need. Nevertheless, well-trained personnel, reliable registries and better patient follow-up would improve outcomes in low-income Asian countries.
Keywords: Asia; Cost of care; Economics; End-stage renal disease; Hemodialysis.
Figures
References
-
- Asia Population 2015 - World Population Review. Available at http://worldpopulationreview.com/continents/asia-population/ (accessed October 2, 2015).
-
- Jones CA, Krolewski AS, Rogus J, et al. Epidemic of end-stage renal disease in people with diabetes in the United States population: do we know the cause? Kidney Int. 2005;67:1684–1691. - PubMed
-
- Meguid El Nahas A, Bello AK. Chronic kidney disease: the global challenge. Lancet. 2005;365:331–340. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
