

Determining Risk of Falls in Community Dwelling Older Adults: A Systematic Review and Meta-analysis Using Posttest Probability
- PMID: 27537070
- PMCID: PMC5158094
- DOI: 10.1519/JPT.0000000000000099
Determining Risk of Falls in Community Dwelling Older Adults: A Systematic Review and Meta-analysis Using Posttest Probability
Abstract
Background: Falls and their consequences are significant concerns for older adults, caregivers, and health care providers. Identification of fall risk is crucial for appropriate referral to preventive interventions. Falls are multifactorial; no single measure is an accurate diagnostic tool. There is limited information on which history question, self-report measure, or performance-based measure, or combination of measures, best predicts future falls.
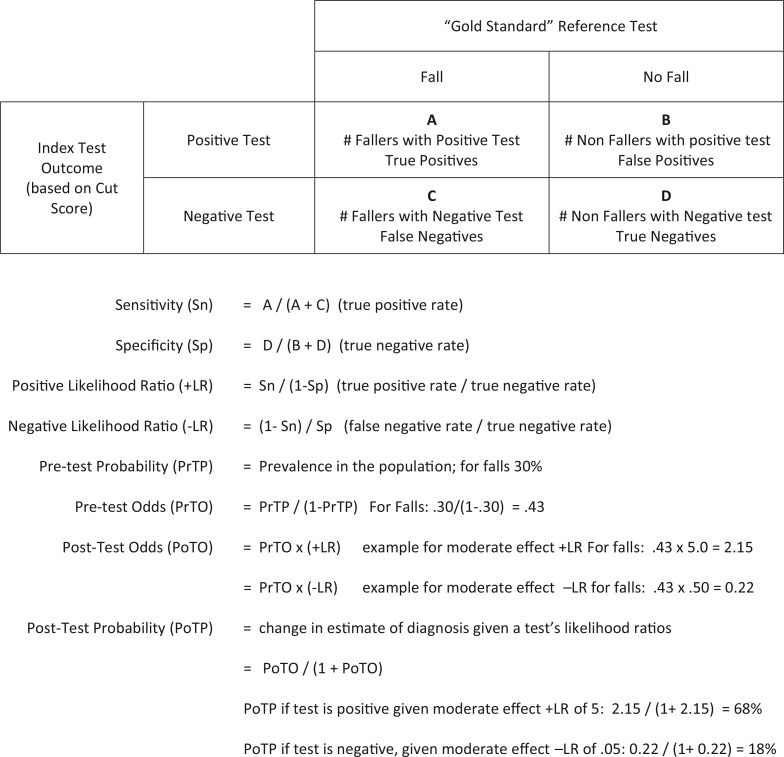
Purpose: First, to evaluate the predictive ability of history questions, self-report measures, and performance-based measures for assessing fall risk of community-dwelling older adults by calculating and comparing posttest probability (PoTP) values for individual test/measures. Second, to evaluate usefulness of cumulative PoTP for measures in combination.
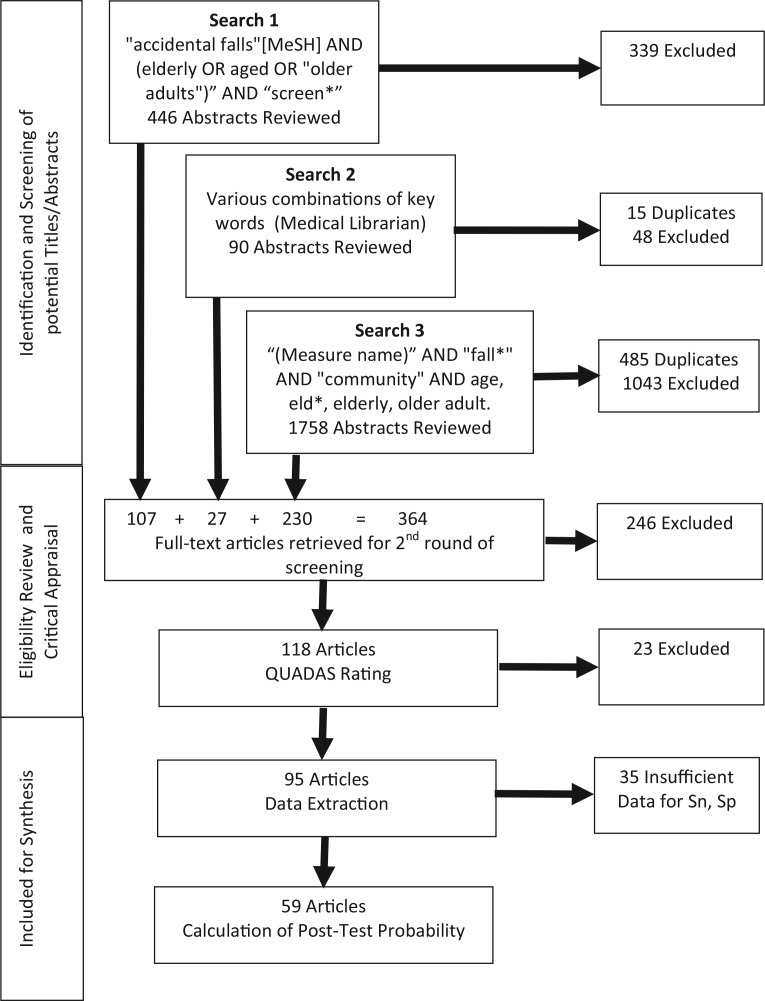
Data sources: To be included, a study must have used fall status as an outcome or classification variable, have a sample size of at least 30 ambulatory community-living older adults (≥65 years), and track falls occurrence for a minimum of 6 months. Studies in acute or long-term care settings, as well as those including participants with significant cognitive or neuromuscular conditions related to increased fall risk, were excluded. Searches of Medline/PubMED and Cumulative Index of Nursing and Allied Health (CINAHL) from January 1990 through September 2013 identified 2294 abstracts concerned with fall risk assessment in community-dwelling older adults.
Study selection: Because the number of prospective studies of fall risk assessment was limited, retrospective studies that classified participants (faller/nonfallers) were also included. Ninety-five full-text articles met inclusion criteria; 59 contained necessary data for calculation of PoTP. The Quality Assessment Tool for Diagnostic Accuracy Studies (QUADAS) was used to assess each study's methodological quality.
Data extraction: Study design and QUADAS score determined the level of evidence. Data for calculation of sensitivity (Sn), specificity (Sp), likelihood ratios (LR), and PoTP values were available for 21 of 46 measures used as search terms. An additional 73 history questions, self-report measures, and performance-based measures were used in included articles; PoTP values could be calculated for 35.
Data synthesis: Evidence tables including PoTP values were constructed for 15 history questions, 15 self-report measures, and 26 performance-based measures. Recommendations for clinical practice were based on consensus.
Limitations: Variations in study quality, procedures, and statistical analyses challenged data extraction, interpretation, and synthesis. There was insufficient data for calculation of PoTP values for 63 of 119 tests.
Conclusions: No single test/measure demonstrated strong PoTP values. Five history questions, 2 self-report measures, and 5 performance-based measures may have clinical usefulness in assessing risk of falling on the basis of cumulative PoTP. Berg Balance Scale score (≤50 points), Timed Up and Go times (≥12 seconds), and 5 times sit-to-stand times (≥12) seconds are currently the most evidence-supported functional measures to determine individual risk of future falls. Shortfalls identified during review will direct researchers to address knowledge gaps.
Figures
References
-
- Stevens JA. Falls among older adults—risk factors and prevention strategies. Falls Free: Promoting a National Falls Prevention Action Plan. Washington, DC: The National Council on the Aging; 2005.
-
- Denkinger MD, Lukas A, Nikolaus T, Hauer K. Factors associated with fear of falling and associated activity restriction in community-dwelling older adults: a systematic review. Am J Geriatr Psychiatry. 2014;23(1):72–86. - PubMed
-
- Allison LK, Painter JA, Emory A, et al. Participation restriction, not fear of falling, predicts actual balance and mobility abilities in rural community-dwelling older adults. J Geriatr Phys Ther. 2013;36(1):13–23. - PubMed
-
- Centers for Disease Control and Prevention. Older Adults Falls Data & Statistics. http://www.cdc.gov/homeandrecreationalsafety/Falls/data.html. Accessed May 8, 2014
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
