

Creatine kinase in the U.S. population: Impact of demographics, comorbidities, and body composition on the normal range
- PMID: 27537560
- PMCID: PMC5370787
- DOI: 10.1097/MD.0000000000004344
Creatine kinase in the U.S. population: Impact of demographics, comorbidities, and body composition on the normal range
Abstract
Background: Creatine kinase (CK) values are a critical part of the workup of suspected myopathies and are often assessed in patients that develop myalgia on statin therapy. CK elevations may influence the initiation and cessation of statin treatment, and incidentally discovered CK elevation may lead to further testing. A number of factors influence CK levels in healthy patients, but current reference ranges do not incorporate important influencers of CK such as race. Objectives of this study were to evaluate clinical factors associated with CK among healthy individuals and to develop practical reference ranges for important subgroups to improve test interpretation.
Methods: CK was evaluated in nonpregnant participants ≥20 years old from the cross-sectional National Health and Nutrition Examination Survey (NHANES) 2011-2014. Linear and logistic regression stratified by sex identified clinical factors associated with CK levels. Adjustment for anthropomorphic measures assessed whether age and race-ethnicity differences in CK were explained by differences in body composition. The 95th and 97.5th percentiles of CK in sex/race-ethnicity subgroups were calculated, excluding patients with recent strenuous exercise.
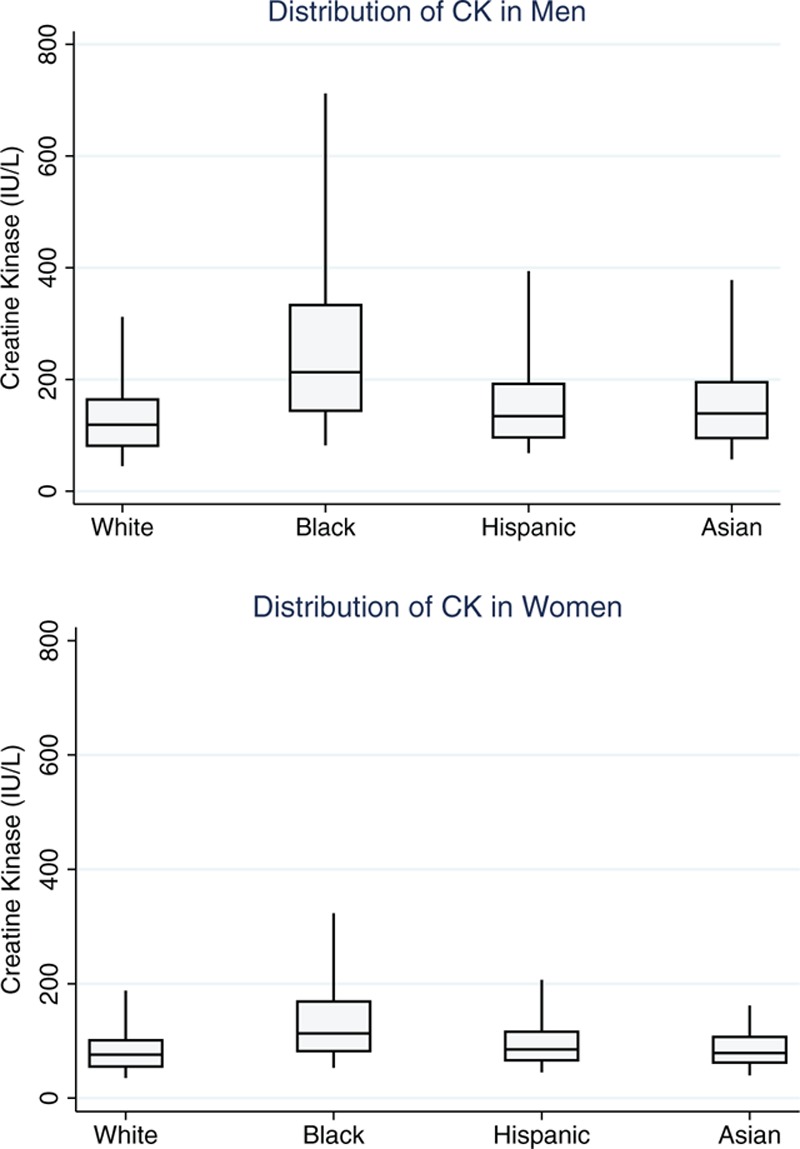
Results: A total of 10,096 nonpregnant adults were studied. Black race was strongly associated with CK. The odds ratio of having an abnormal CK for black women was 5.08 (95% CI 3.65-7.08) and for black men was 8.39 (95% CI 6.11-11.52). CK was substantially lower in older men. Differences in CK by age but not race-ethnicity were largely explained by body composition. Women with low body mass index were less likely to have an elevated CK, and overweight or obese men had an almost 2-fold greater odds of having an elevated CK. The 97.5th percentile of CK was 382 (95% CI 295-469) in white men, 1001 (95% CI 718-1284) in black men, 295 (95% CI 216-374) in white women, and 487 (95% CI 310-664) in black women.
Conclusion: CK is substantially higher in men and in black patients. Differences in body size and composition are also important but do not explain racial differences in CK. The 95th and 97.5th percentiles in sex and race-ethnicity subgroups provide a practical guide for clinicians interpreting CK values.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
References
-
- Stone NJ, Robinson JG, Lichtenstein AH, et al. 2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol 2014; 63 (25 Pt B):2889–2934. - PubMed
-
- Ganga HV, Slim HB, Thompson PD. A systematic review of statin-induced muscle problems in clinical trials. Am Heart J 2014; 168:6–15. - PubMed
-
- Meltzer HY. Factors affecting serum creatine phosphokinase levels in the general population: the role of race, activity and age. Clin Chim Acta Int J Clin Chem 1971; 33:165–172. - PubMed
-
- Wong ET, Cobb C, Umehara MK, et al. Heterogeneity of serum creatine kinase activity among racial and gender groups of the population. Am J Clin Pathol 1983; 79:582–586. - PubMed
-
- Black HR, Quallich H, Gareleck CB. Racial differences in serum creatine kinase levels. Am J Med 1986; 81:479–487. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
