

Superior outcomes of kidney transplantation compared with dialysis: An optimal matched analysis of a national population-based cohort study between 2005 and 2008 in Korea
- PMID: 27537562
- PMCID: PMC5370789
- DOI: 10.1097/MD.0000000000004352
Superior outcomes of kidney transplantation compared with dialysis: An optimal matched analysis of a national population-based cohort study between 2005 and 2008 in Korea
Abstract
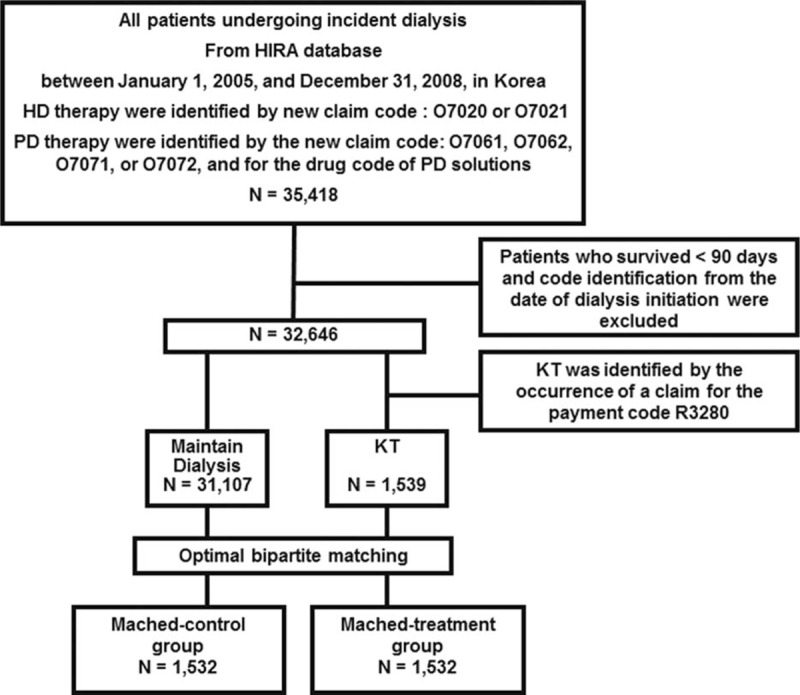
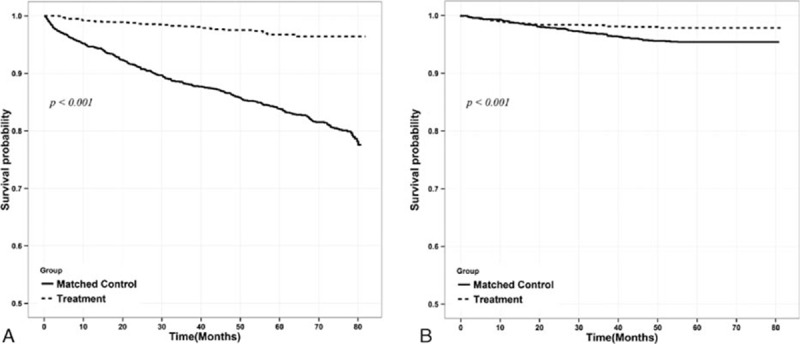
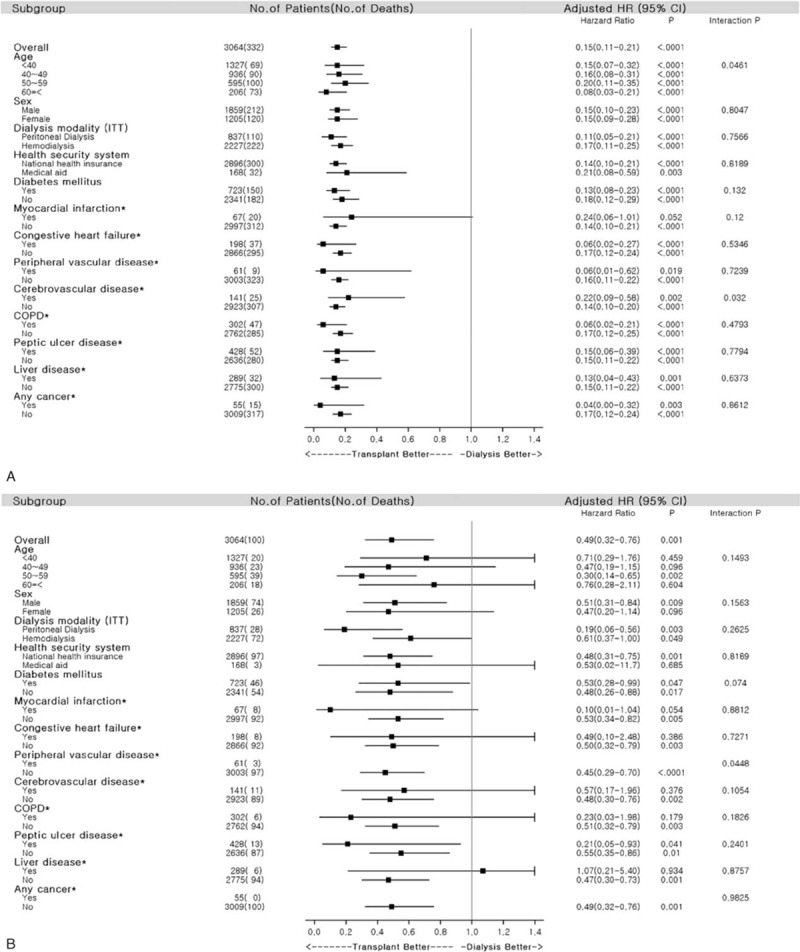
Data regarding kidney transplantation (KT) and dialysis outcomes are rare in Asian populations. In the present study, we evaluated the clinical outcomes associated with KT using claims data from the Korean national public health insurance program. Among the 35,418 adult patients with incident dialysis treated between 2005 and 2008 in Korea, 1539 underwent KT. An optimal balanced risk set matching was attempted to compare the transplant group with the control group in terms of the overall survival and major adverse cardiac event-free survival. Before matching, the dialysis group was older and had more comorbidities. After matching, there were no differences in age, sex, dialysis modalities, or comorbidities. Patient survival was significantly better in the transplant group than in the matched control group (P < 0.001). In addition, the transplant group showed better major adverse cardiac event-free survival than the dialysis group (P < 0.001; hazard ratio, 0.49; 95% confidence interval, 0.32-0.75). Korean patients with incident dialysis who underwent long-term dialysis had significantly more cardiovascular events and higher all-cause mortality rates than those who underwent KT. Thus, KT should be more actively recommended in Korean populations.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
References
-
- Locatelli F, Del Vecchio L, Manzoni C. Morbidity and mortality on maintenance haemodialysis. Nephron 1998; 80:380–400. - PubMed
-
- Collins AJ, Foley RN, Gilbertson DT, et al. The state of chronic kidney disease, ESRD, and morbidity and mortality in the first year of dialysis. Clin J Am Soc Nephrol 2009; 4:S5–S11. - PubMed
-
- Laupacis A, Keown P, Pus N, et al. A study of the quality of life and cost–utility of renal transplantation. Kidney Int 1996; 50:235–242. - PubMed
-
- Wolfe RA, Ashby VB, Milford EL, et al. Comparison of mortality in all patients on dialysis, patients on dialysis awaiting transplantation, and recipients of a first cadaveric transplant. N Engl J Med 1999; 341:1725–1730. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
