

Live volumetric (4D) visualization and guidance of in vivo human ophthalmic surgery with intraoperative optical coherence tomography
- PMID: 27538478
- PMCID: PMC4990849
- DOI: 10.1038/srep31689
Live volumetric (4D) visualization and guidance of in vivo human ophthalmic surgery with intraoperative optical coherence tomography
Abstract
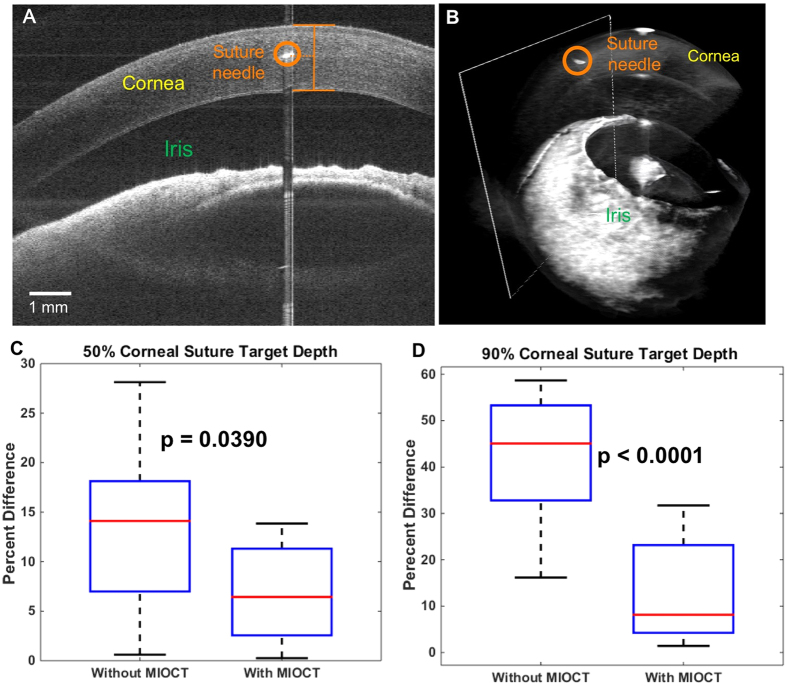
Minimally-invasive microsurgery has resulted in improved outcomes for patients. However, operating through a microscope limits depth perception and fixes the visual perspective, which result in a steep learning curve to achieve microsurgical proficiency. We introduce a surgical imaging system employing four-dimensional (live volumetric imaging through time) microscope-integrated optical coherence tomography (4D MIOCT) capable of imaging at up to 10 volumes per second to visualize human microsurgery. A custom stereoscopic heads-up display provides real-time interactive volumetric feedback to the surgeon. We report that 4D MIOCT enhanced suturing accuracy and control of instrument positioning in mock surgical trials involving 17 ophthalmic surgeons. Additionally, 4D MIOCT imaging was performed in 48 human eye surgeries and was demonstrated to successfully visualize the pathology of interest in concordance with preoperative diagnosis in 93% of retinal surgeries and the surgical site of interest in 100% of anterior segment surgeries. In vivo 4D MIOCT imaging revealed sub-surface pathologic structures and instrument-induced lesions that were invisible through the operating microscope during standard surgical maneuvers. In select cases, 4D MIOCT guidance was necessary to resolve such lesions and prevent post-operative complications. Our novel surgical visualization platform achieves surgeon-interactive 4D visualization of live surgery which could expand the surgeon's capabilities.
Conflict of interest statement
At the time this study was conducted, Dr. Izatt was Chairman and Chief Scientific Advisor for Bioptigen, Inc. (since acquired by Leica Microsystems) and had corporate, equity, and intellectual property interests (including royalties) in this company. O.M.C.Z., B.K., C.V., L.S., S.F., A.N.K., C.A.T. and J.A.T. are inventors on issued and pending patents pertaining to the technology described in this paper.
Figures







Similar articles
-
Optical Coherence Tomography for Retinal Surgery: Perioperative Analysis to Real-Time Four-Dimensional Image-Guided Surgery.Invest Ophthalmol Vis Sci. 2016 Jul 1;57(9):OCT37-50. doi: 10.1167/iovs.16-19277. Invest Ophthalmol Vis Sci. 2016. PMID: 27409495 Free PMC article. Review.
-
Preclinical evaluation and intraoperative human retinal imaging with a high-resolution microscope-integrated spectral domain optical coherence tomography device.Retina. 2013 Jul-Aug;33(7):1328-37. doi: 10.1097/IAE.0b013e3182831293. Retina. 2013. PMID: 23538579 Free PMC article.
-
Determination of feasibility and utility of microscope-integrated optical coherence tomography during ophthalmic surgery: the DISCOVER Study RESCAN Results.JAMA Ophthalmol. 2015 Oct;133(10):1124-32. doi: 10.1001/jamaophthalmol.2015.2376. JAMA Ophthalmol. 2015. PMID: 26226623 Free PMC article.
-
Four-dimensional microscope- integrated optical coherence tomography to enhance visualization in glaucoma surgeries.Indian J Ophthalmol. 2017 Jan;65(1):57-59. doi: 10.4103/ijo.IJO_412_16. Indian J Ophthalmol. 2017. PMID: 28300743 Free PMC article.
-
[Intraoperative OCT in ophthalmic microsurgery].Ophthalmologe. 2016 May;113(5):435-42. doi: 10.1007/s00347-016-0250-8. Ophthalmologe. 2016. PMID: 27126797 Review. German.
Cited by
-
Real-time corneal segmentation and 3D needle tracking in intrasurgical OCT.Biomed Opt Express. 2018 May 21;9(6):2716-2732. doi: 10.1364/BOE.9.002716. eCollection 2018 Jun 1. Biomed Opt Express. 2018. PMID: 30258685 Free PMC article.
-
Optical Coherence Tomography Guided Robotic Needle Insertion for Deep Anterior Lamellar Keratoplasty.IEEE Trans Biomed Eng. 2020 Jul;67(7):2073-2083. doi: 10.1109/TBME.2019.2954505. Epub 2019 Nov 20. IEEE Trans Biomed Eng. 2020. PMID: 31751219 Free PMC article.
-
Endoscopic vitreoretinal surgery: principles, applications and new directions.Int J Retina Vitreous. 2019 Jun 18;5:15. doi: 10.1186/s40942-019-0165-z. eCollection 2019. Int J Retina Vitreous. 2019. PMID: 31236288 Free PMC article. Review.
-
Optical coherence tomography for thyroid pathology: 3D analysis of tissue microstructure.Biomed Opt Express. 2020 Jul 9;11(8):4130-4149. doi: 10.1364/BOE.394296. eCollection 2020 Aug 1. Biomed Opt Express. 2020. PMID: 32923033 Free PMC article.
-
Advances in multimodal imaging in ophthalmology.Ther Adv Ophthalmol. 2021 Mar 19;13:25158414211002400. doi: 10.1177/25158414211002400. eCollection 2021 Jan-Dec. Ther Adv Ophthalmol. 2021. PMID: 35187398 Free PMC article. Review.
References
-
- Daniel R. K. Microsurgery: Through the looking glass. N. Engl. J. Med. 300, 1251–1257 (1979). - PubMed
-
- Singh M. & Saxena A. Microsurgery: A Useful and Versatile Tool in Surgical Field. Surg. Curr. Res. 04, 9–11 (2014).
-
- Reznick R. K. & MacRae H. Teaching Surgical Skills - Changes in the Wind. N. Engl. J. Med. 355, 2664–9 (2006). - PubMed
-
- Ramachandran S., Ghanem A. M. & Myers S. R. Assessment of microsurgery competency-where are we now? Microsurgery 33, 406–415 (2013). - PubMed
-
- Institute N. E. Age-related Eye Disease Study. (2013).
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
