

Dynamic clonal equilibrium and predetermined cancer risk in Barrett's oesophagus
- PMID: 27538785
- PMCID: PMC4992167
- DOI: 10.1038/ncomms12158
Dynamic clonal equilibrium and predetermined cancer risk in Barrett's oesophagus
Abstract
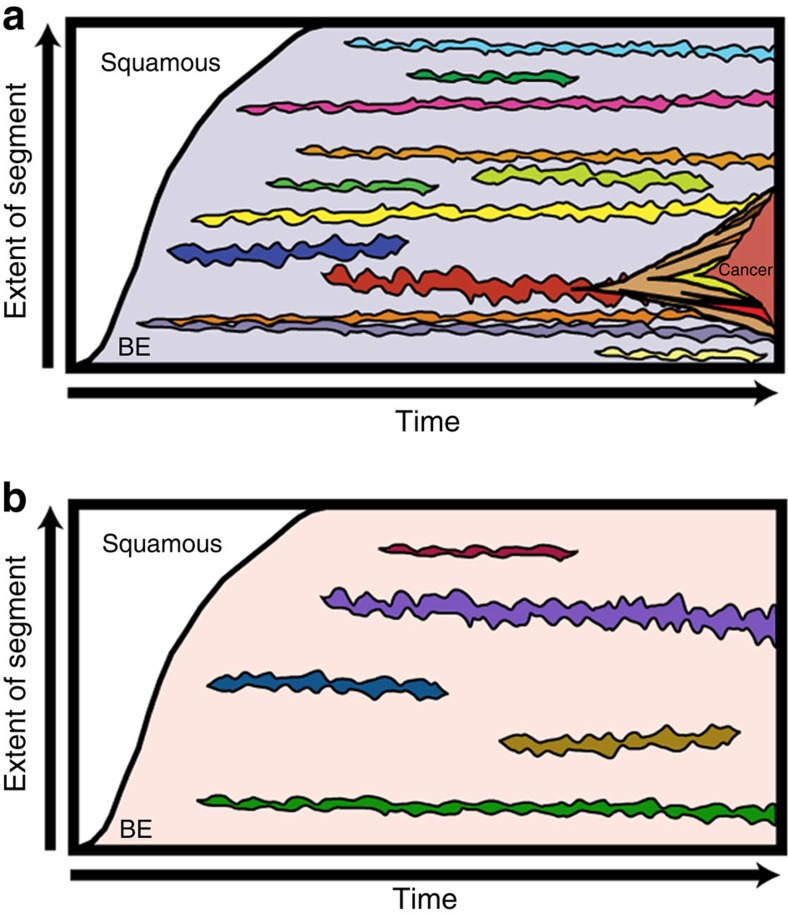
Surveillance of Barrett's oesophagus allows us to study the evolutionary dynamics of a human neoplasm over time. Here we use multicolour fluorescence in situ hybridization on brush cytology specimens, from two time points with a median interval of 37 months in 195 non-dysplastic Barrett's patients, and a third time point in a subset of 90 patients at a median interval of 36 months, to study clonal evolution at single-cell resolution. Baseline genetic diversity predicts progression and remains in a stable dynamic equilibrium over time. Clonal expansions are rare, being detected once every 36.8 patient years, and growing at an average rate of 1.58 cm(2) (95% CI: 0.09-4.06) per year, often involving the p16 locus. This suggests a lack of strong clonal selection in Barrett's and that the malignant potential of 'benign' Barrett's lesions is predetermined, with important implications for surveillance programs.
Conflict of interest statement
Dr Krishnadath has a patent 10999US01 issued: US/23.09.11/USP201161538291, Materials and methods for prognosis of progression of Barrett's oesophagus. The remaining authors declare no conflict of interests.
Figures




References
-
- Nowell P. C. The clonal evolution of tumor cell populations. Science 194, 23–28 (1976). - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
