

Canagliflozin Slows Progression of Renal Function Decline Independently of Glycemic Effects
- PMID: 27539604
- PMCID: PMC5198289
- DOI: 10.1681/ASN.2016030278
Canagliflozin Slows Progression of Renal Function Decline Independently of Glycemic Effects
Abstract
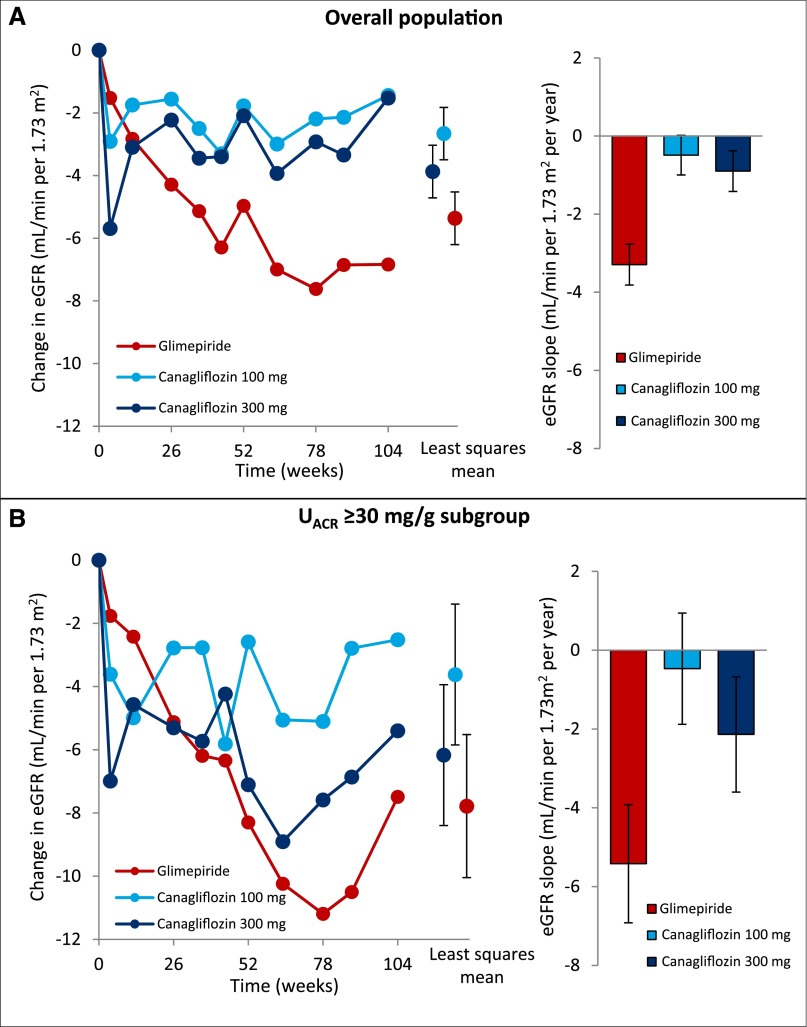
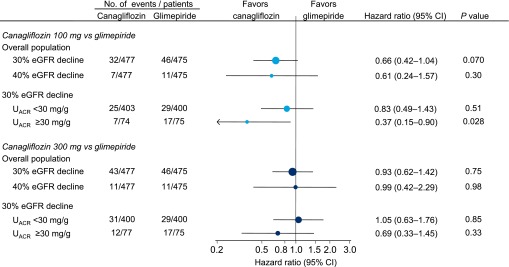
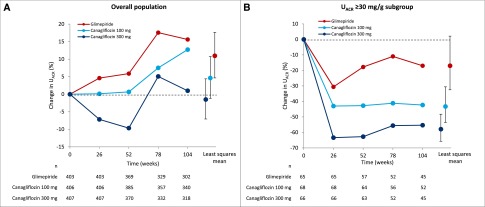
Sodium-glucose cotransporter 2 inhibition with canagliflozin decreases HbA1c, body weight, BP, and albuminuria, implying that canagliflozin confers renoprotection. We determined whether canagliflozin decreases albuminuria and reduces renal function decline independently of its glycemic effects in a secondary analysis of a clinical trial in 1450 patients with type 2 diabetes receiving metformin and randomly assigned to either once-daily canagliflozin 100 mg, canagliflozin 300 mg, or glimepiride uptitrated to 6-8 mg. End points were annual change in eGFR and albuminuria over 2 years of follow-up. Glimepiride, canagliflozin 100 mg, and canagliflozin 300 mg groups had eGFR declines of 3.3 ml/min per 1.73 m2 per year (95% confidence interval [95% CI], 2.8 to 3.8), 0.5 ml/min per 1.73 m2 per year (95% CI, 0.0 to 1.0), and 0.9 ml/min per 1.73 m2 per year (95% CI, 0.4 to 1.4), respectively (P<0.01 for each canagliflozin group versus glimepiride). In the subgroup of patients with baseline urinary albumin-to-creatinine ratio ≥30 mg/g, urinary albumin-to-creatinine ratio decreased more with canagliflozin 100 mg (31.7%; 95% CI, 8.6% to 48.9%; P=0.01) or canagliflozin 300 mg (49.3%; 95% CI, 31.9% to 62.2%; P<0.001) than with glimepiride. Patients receiving glimepiride, canagliflozin 100 mg, or canagliflozin 300 mg had reductions in HbA1c of 0.81%, 0.82%, and 0.93%, respectively, at 1 year and 0.55%, 0.65%, and 0.74%, respectively, at 2 years. In conclusion, canagliflozin 100 or 300 mg/d, compared with glimepiride, slowed the progression of renal disease over 2 years in patients with type 2 diabetes, and canagliflozin may confer renoprotective effects independently of its glycemic effects.
Keywords: SGLT2; canagliflozin; diabetic nephropathy; renal function.
Copyright © 2016 by the American Society of Nephrology.
Figures
Comment in
-
SGLT2 Inhibitors-Sweet Success for Diabetic Kidney Disease?J Am Soc Nephrol. 2017 Jan;28(1):7-10. doi: 10.1681/ASN.2016060650. Epub 2016 Aug 18. J Am Soc Nephrol. 2017. PMID: 27539605 Free PMC article. No abstract available.
References
-
- American Diabetes Association : Standards of medical care in diabetes–2015. Diabetes Care 38[Suppl]: S1–S93, 2015
-
- Mudaliar S, Polidori D, Zambrowicz B, Henry RR: Sodium-glucose cotransporter inhibitors: effects on renal and intestinal glucose transport: from bench to bedside. Diabetes Care 38: 2344–2353, 2015 - PubMed
-
- Cefalu WT, Leiter LA, Yoon KH, Arias P, Niskanen L, Xie J, Balis DA, Canovatchel W, Meininger G: Efficacy and safety of canagliflozin versus glimepiride in patients with type 2 diabetes inadequately controlled with metformin (CANTATA-SU): 52 week results from a randomised, double-blind, phase 3 non-inferiority trial. Lancet 382: 941–950, 2013 - PubMed
-
- Brewster UC, Setaro JF, Perazella MA: The renin-angiotensin-aldosterone system: cardiorenal effects and implications for renal and cardiovascular disease states. Am J Med Sci 326: 15–24, 2003 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
