

Low-grade inflammation as a key mediator of the pathogenesis of osteoarthritis
- PMID: 27539668
- PMCID: PMC5500215
- DOI: 10.1038/nrrheum.2016.136
Low-grade inflammation as a key mediator of the pathogenesis of osteoarthritis
Abstract
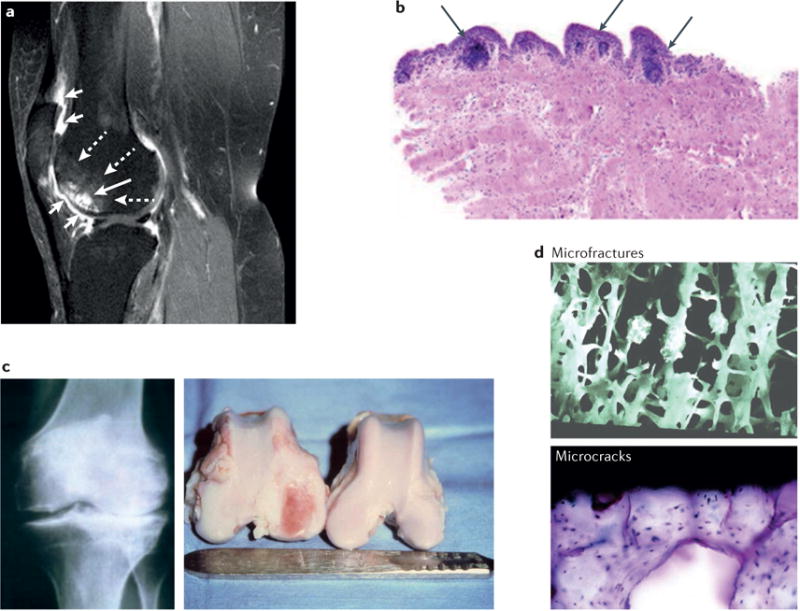
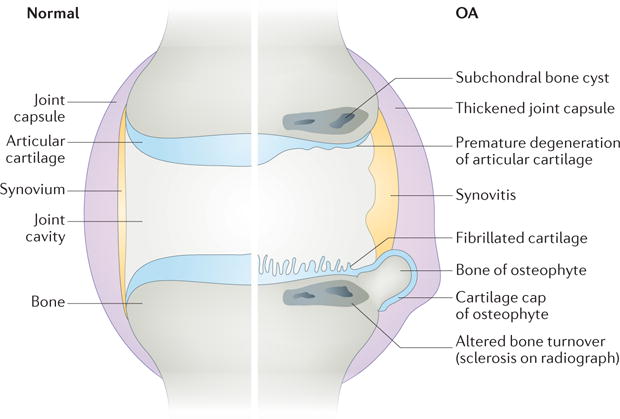
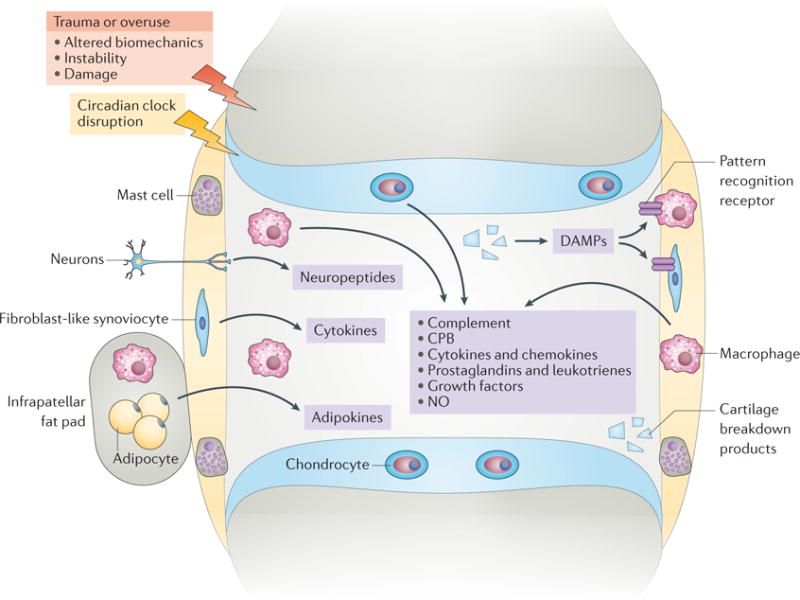
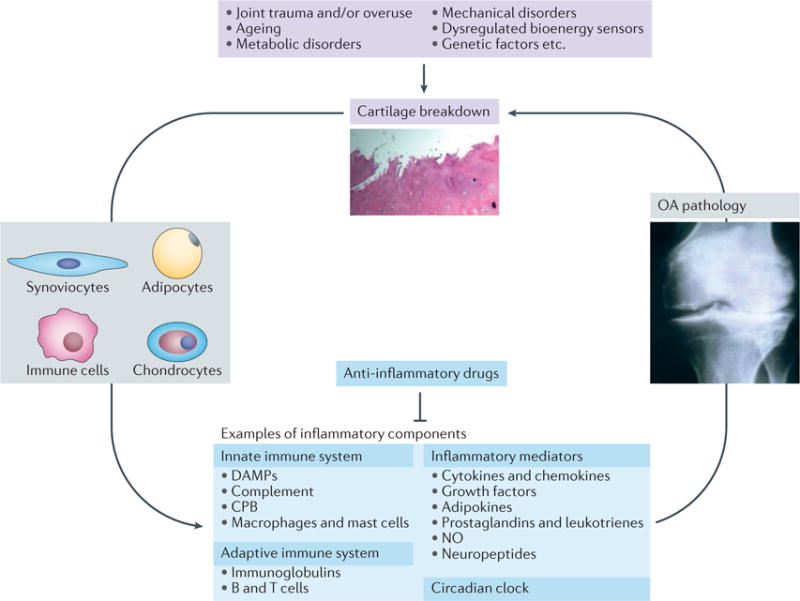
Osteoarthritis (OA) has long been viewed as a degenerative disease of cartilage, but accumulating evidence indicates that inflammation has a critical role in its pathogenesis. Furthermore, we now appreciate that OA pathogenesis involves not only breakdown of cartilage, but also remodelling of the underlying bone, formation of ectopic bone, hypertrophy of the joint capsule, and inflammation of the synovial lining. That is, OA is a disorder of the joint as a whole, with inflammation driving many pathologic changes. The inflammation in OA is distinct from that in rheumatoid arthritis and other autoimmune diseases: it is chronic, comparatively low-grade, and mediated primarily by the innate immune system. Current treatments for OA only control the symptoms, and none has been FDA-approved for the prevention or slowing of disease progression. However, increasing insight into the inflammatory underpinnings of OA holds promise for the development of new, disease-modifying therapies. Indeed, several anti-inflammatory therapies have shown promise in animal models of OA. Further work is needed to identify effective inhibitors of the low-grade inflammation in OA, and to determine whether therapies that target this inflammation can prevent or slow the development and progression of the disease.
Conflict of interest statement
J.S. is an employee of AbbVie. All other authors declare no competing interests.
Figures
References
-
- Felson DT. Clinical practice. Osteoarthritis of the knee. N Engl J Med. 2006;354:841–848. - PubMed
-
- Felson DT, et al. Osteoarthritis: new insights. Part 2: treatment approaches. Ann Intern Med. 2000;133:726–737. - PubMed
-
- Blagojevic M, Jinks C, Jeffery A, Jordan K. P Risk factors for onset of osteoarthritis of the knee in older adults: a systematic review and meta-analysis. Osteoarthritis Cartilage. 2010;18:24–33. - PubMed
-
- Zhuo Q, Yang W, Chen J, Wang Y. Metabolic syndrome meets osteoarthritis. Nat Rev Rheumatol. 2012;8:729–737. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
