

Data feedback and behavioural change intervention to improve primary care prescribing safety (EFIPPS): multicentre, three arm, cluster randomised controlled trial
- PMID: 27540041
- PMCID: PMC4990081
- DOI: 10.1136/bmj.i4079
Data feedback and behavioural change intervention to improve primary care prescribing safety (EFIPPS): multicentre, three arm, cluster randomised controlled trial
Abstract
Objective: To evaluate the effectiveness of feedback on safety of prescribing compared with moderately enhanced usual care.
Design: Three arm, highly pragmatic cluster randomised trial.
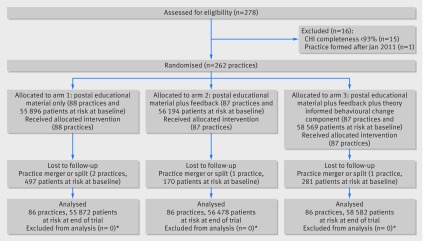
Setting and participants: 262/278 (94%) primary care practices in three Scottish health boards.
Interventions: Practices were randomised to: "usual care," consisting of emailed educational material with support for searching to identify patients (88 practices at baseline, 86 analysed); usual care plus feedback on practice's high risk prescribing sent quarterly on five occasions (87 practices, 86 analysed); or usual care plus the same feedback incorporating a behavioural change component (87 practices, 86 analysed).
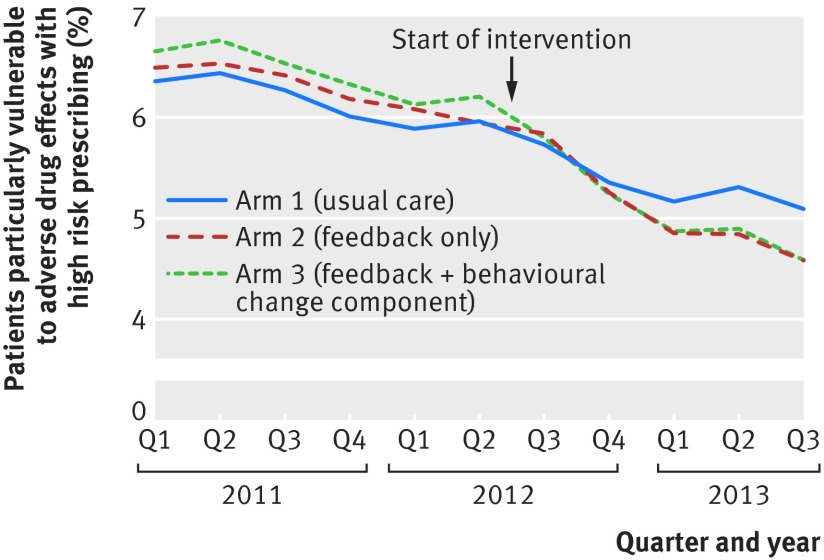
Main outcome measures: The primary outcome was a patient level composite of six prescribing measures relating to high risk use of antipsychotics, non-steroidal anti-inflammatories, and antiplatelets. Secondary outcomes were the six individual measures. The primary analysis compared high risk prescribing in the two feedback arms against usual care at 15 months. Secondary analyses examined immediate change and change in trend of high risk prescribing associated with implementation of the intervention within each arm.
Results: In the primary analysis, high risk prescribing as measured by the primary outcome fell from 6.0% (3332/55 896) to 5.1% (2845/55 872) in the usual care arm, compared with 5.9% (3341/56 194) to 4.6% (2587/56 478) in the feedback only arm (odds ratio 0.88 (95% confidence interval 0.80 to 0.96) compared with usual care; P=0.007) and 6.2% (3634/58 569) to 4.6% (2686/58 582) in the feedback plus behavioural change component arm (0.86 (0.78 to 0.95); P=0.002). In the pre-specified secondary analysis of change in trend within each arm, the usual care educational intervention had no effect on the existing declining trend in high risk prescribing. Both types of feedback were associated with significantly more rapid decline in high risk prescribing after the intervention compared with before.
Conclusions: Feedback of prescribing safety data was effective at reducing high risk prescribing. The intervention would be feasible to implement at scale in contexts where electronic health records are in general use.Trial registration Clinical trials NCT01602705.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at
Figures
References
-
- Pirmohamed M, James S, Meakin S, et al. Adverse drug reactions as cause of admission to hospital: prospective analysis of 18 820 patients. BMJ 2004;329:15-9. 10.1136/bmj.329.7456.15 pmid:15231615. - DOI - PMC - PubMed
-
- Gandhi TK, Weingart SN, Borus J, et al. Adverse drug events in ambulatory care. N Engl J Med 2003;348:1556-64. 10.1056/NEJMsa020703 pmid:12700376. - DOI - PubMed
-
- Gurwitz JH, Field TS, Harrold LR, et al. Incidence and preventability of adverse drug events among older persons in the ambulatory setting. JAMA 2003;289:1107-16. 10.1001/jama.289.9.1107 pmid:12622580. - DOI - PubMed
-
- Howard RL, Avery AJ, Slavenburg S, et al. Which drugs cause preventable admissions to hospital? A systematic review. Br J Clin Pharmacol 2007;63:136-47. 10.1111/j.1365-2125.2006.02698.x pmid:16803468. - DOI - PMC - PubMed
-
- Banerjee S. The use of antipsychotic medication for people with dementia: time for action.Department of Health, 2009.
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical