

Prematurity and Genetic Testing for Neonatal Diabetes
- PMID: 27540106
- PMCID: PMC5049686
- DOI: 10.1542/peds.2015-3926
Prematurity and Genetic Testing for Neonatal Diabetes
Abstract
Background: Hyperglycemia in premature infants is usually thought to reflect inadequate pancreatic development rather than monogenic neonatal diabetes. No studies, to our knowledge, have investigated the prevalence of monogenic forms of diabetes in preterm infants.
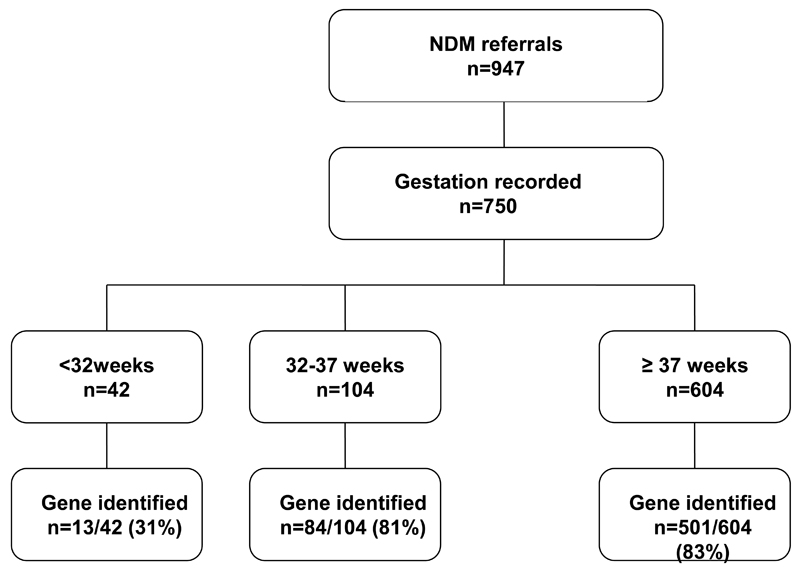
Methods: We studied 750 patients with diabetes diagnosed before 6 months of age. We compared the genetic etiology and clinical characteristics of 146 preterm patients born <37 weeks and compared them with 604 born ≥37 weeks.
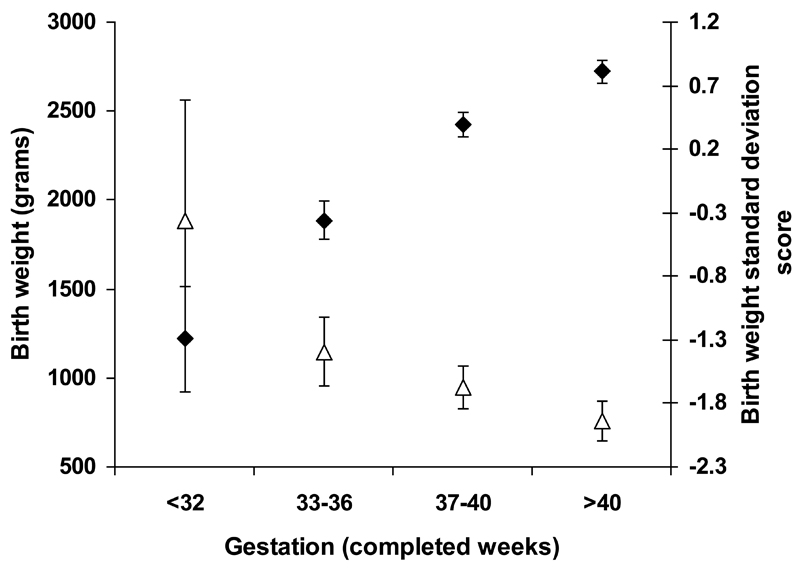
Results: A genetic etiology was found in 97/146 (66%) preterm infants compared with 501/604 (83%) born ≥37weeks, P < .0001. Chromosome 6q24 imprinting abnormalities (27% vs 12%, P = .0001) and GATA6 mutations (9% vs 2%, P = .003) occurred more commonly in preterm than term infants while mutations in KCNJ11 were less common (21 vs 34%, P = .008). Preterm patients with an identified mutation were diagnosed later than those without an identified mutation (median [interquartile range] 35 [34 to 36] weeks vs 31 [28 to 36] weeks, P < .0001). No difference was seen in other clinical characteristics of preterm patients with and without an identified mutation including age of presentation, birth weight, and time to referral.
Conclusions: Patients with neonatal diabetes due to a monogenic etiology can be born preterm, especially those with 6q24 abnormalities or GATA6 mutations. A genetic etiology is more likely in patients with less severe prematurity (>32 weeks). Prematurity should not prevent referral for genetic testing as 37% have a potassium channel mutation and as a result can get improved control by replacing insulin with sulphonylurea therapy.
Copyright © 2016 by the American Academy of Pediatrics.
Conflict of interest statement
Conflict of Interest. None of the authors have any conflicts of interest to disclose.
Figures
References
-
- Martin JA, Hamilton BE, Ventura SJ, et al. Births: final data for 2009. Natl Vital Stat Rep. 2011;60(1):1–70. - PubMed
-
- Mitanchez-Mokhtari D, Lahlou N, Kieffer F, Magny JF, Roger M, Voyer M. Both relative insulin resistance and defective islet beta-cell processing of proinsulin are responsible for transient hyperglycemia in extremely preterm infants. Pediatrics. 2004;113(3 Pt 1):537–541. - PubMed
-
- Ogilvy-Stuart AL, Beardsall K. Management of aemia in the preterm infant. Arch Dis Child Fetal Neonatal Ed. 2010;95(2):F126–131. - PubMed
-
- Dweck HS, Cassady G. Glucose intolerance in infants of very low birth weight. I. Incidence of hyperglycemia in infants of birth weights 1,100 grams or less. Pediatrics. 1974;53(2):189–195. - PubMed
-
- Louik C, Mitchell AA, Epstein MF, Shapiro S. Risk factors for neonatal hyperglycemia associated with 10% dextrose infusion. Am J Dis Child. 1985;139(8):783–786. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
