

Clinical Impact and Cost-effectiveness of Diagnosing HIV Infection During Early Infancy in South Africa: Test Timing and Frequency
- PMID: 27540110
- PMCID: PMC5079370
- DOI: 10.1093/infdis/jiw379
Clinical Impact and Cost-effectiveness of Diagnosing HIV Infection During Early Infancy in South Africa: Test Timing and Frequency
Abstract
Background: Diagnosis of human immunodeficiency virus (HIV) infection during early infancy (commonly known as "early infant HIV diagnosis" [EID]) followed by prompt initiation of antiretroviral therapy dramatically reduces mortality. EID testing is recommended at 6 weeks of age, but many infant infections are missed.
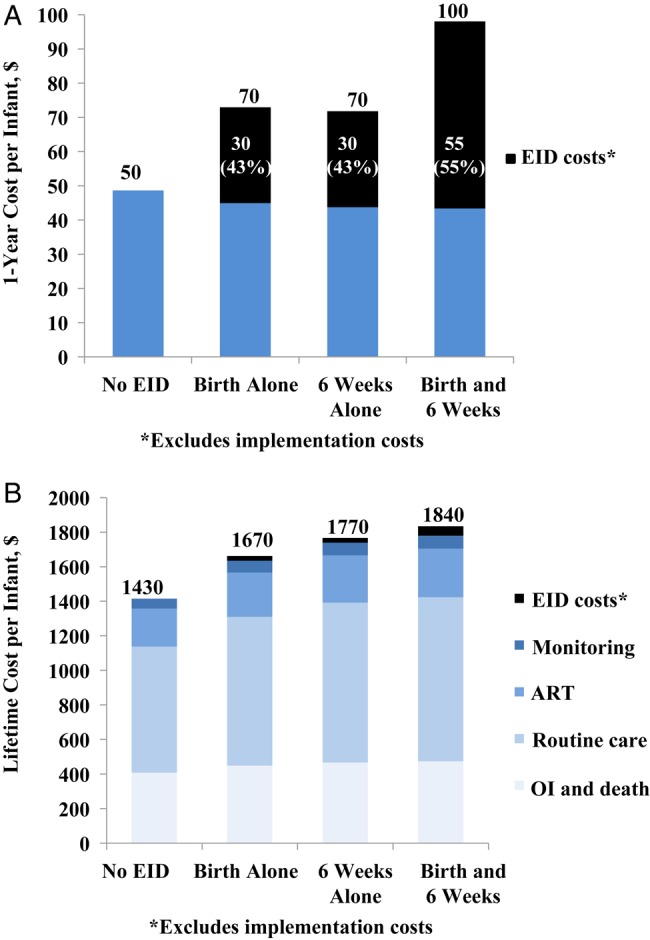
Design/methods: We simulated 4 EID testing strategies for HIV-exposed infants in South Africa: no EID (diagnosis only after illness; hereafter, "no EID"), testing once (at birth alone or at 6 weeks of age alone; hereafter, "birth alone" and "6 weeks alone," respectively), and testing twice (at birth and 6 weeks of age; hereafter "birth and 6 weeks"). We calculated incremental cost-effectiveness ratios (ICERs), using discounted costs and life expectancies for all HIV-exposed (infected and uninfected) infants.
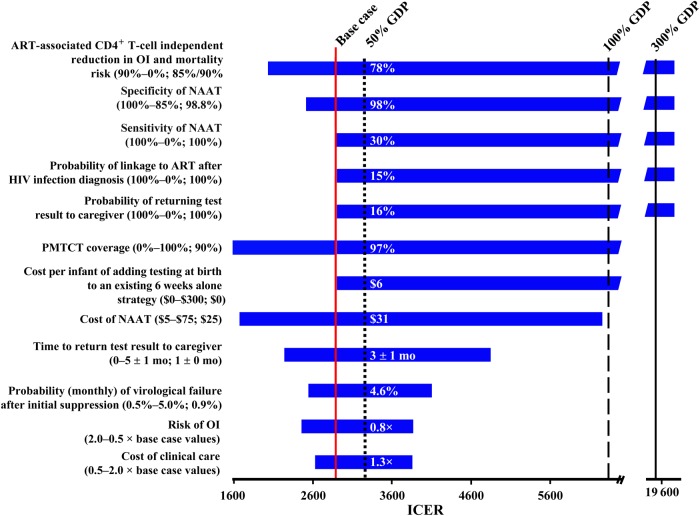
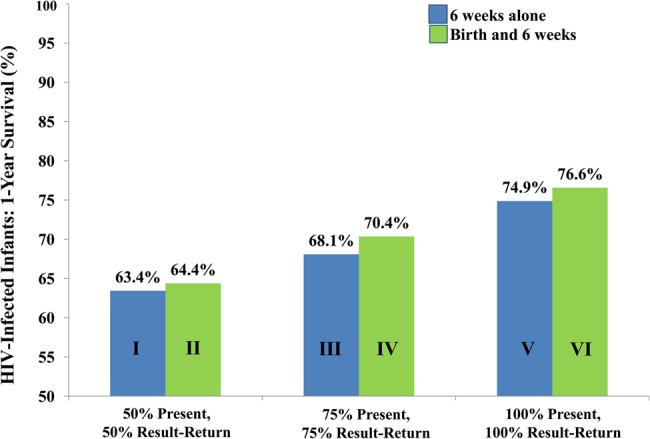
Results: In the base case (guideline-concordant care), the no EID strategy produced a life expectancy of 21.1 years (in the HIV-infected group) and 61.1 years (in the HIV-exposed group); lifetime cost averaged $1430/HIV-exposed infant. The birth and 6 weeks strategy maximized life expectancy (26.5 years in the HIV-infected group and 61.4 years in the HIV-exposed group), costing $1840/infant tested. The ICER of the 6 weeks alone strategy versus the no EID strategy was $1250/year of life saved (19% of South Africa's per capita gross domestic product); the ICER for the birth and 6 weeks strategy versus the 6 weeks alone strategy was $2900/year of life saved (45% of South Africa's per capita gross domestic product). Increasing the proportion of caregivers who receive test results and the linkage of HIV-positive infants to antiretroviral therapy with the 6 weeks alone strategy improved survival more than adding a second test.
Conclusions: EID at birth and 6 weeks improves outcomes and is cost-effective, compared with EID at 6 weeks alone. If scale-up costs are comparable, programs should add birth testing after strengthening 6-week testing programs.
Keywords: birth testing; cost-effectiveness; early infant HIV diagnosis; human immunodeficiency virus; nucleic acid test.
© The Author 2016. Published by Oxford University Press for the Infectious Diseases Society of America. All rights reserved. For permissions, e-mail journals.permissions@oup.com.
Figures
Comment in
-
Diagnosis of HIV Infection During Early Infancy: How Early Is Early Enough?J Infect Dis. 2016 Nov 1;214(9):1294-1296. doi: 10.1093/infdis/jiw383. Epub 2016 Aug 17. J Infect Dis. 2016. PMID: 27540111 No abstract available.
References
-
- World Health Organization (WHO). Progress report on the global plan towards the elimination of new HIV infections among children and keeping their mothers alive. Geneva, Switzerland: WHO, 2015. http://www.unaids.org/sites/default/files/media_asset/JC2774_2015Progres... Accessed 22 March 2016.
-
- Newell ML, Coovadia H, Cortina-Borja M, Rollins N, Gaillard P, Dabis F. Mortality of infected and uninfected infants born to HIV-infected mothers in Africa: a pooled analysis. Lancet 2004; 364:1236–43. - PubMed
-
- Bourne DE, Thompson M, Brody LL et al. . Emergence of a peak in early infant mortality due to HIV/AIDS in South Africa. AIDS 2009; 23:101–6. - PubMed
-
- World Health Organization. Consolidated guidelines on the use of antiretrovirals for the treatment and prevention of HIV infection. Geneva, Switzerland: WHO, 2013. http://www.who.int/hiv/pub/guidelines/arv2013/download/en/index.html Accessed 7 July 2016.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
