

Factors Influencing Disconnection Hyperprolactinemia and Reversal of Serum Prolactin after Pituitary Surgery in a Non-Functioning Pituitary Macroadenoma
- PMID: 27540328
- PMCID: PMC4975579
Factors Influencing Disconnection Hyperprolactinemia and Reversal of Serum Prolactin after Pituitary Surgery in a Non-Functioning Pituitary Macroadenoma
Abstract
Background: To investigate factors influencing disconnection hyperprolactinemia, including tumour volume, degree of pituitary stalk displacement and extent of tumour growth based on a modified Wilson-Hardy classification in a non-functioning pituitary macroadenoma and to confirm reductions in serum prolactin levels after endoscopic transphenoidal surgery.
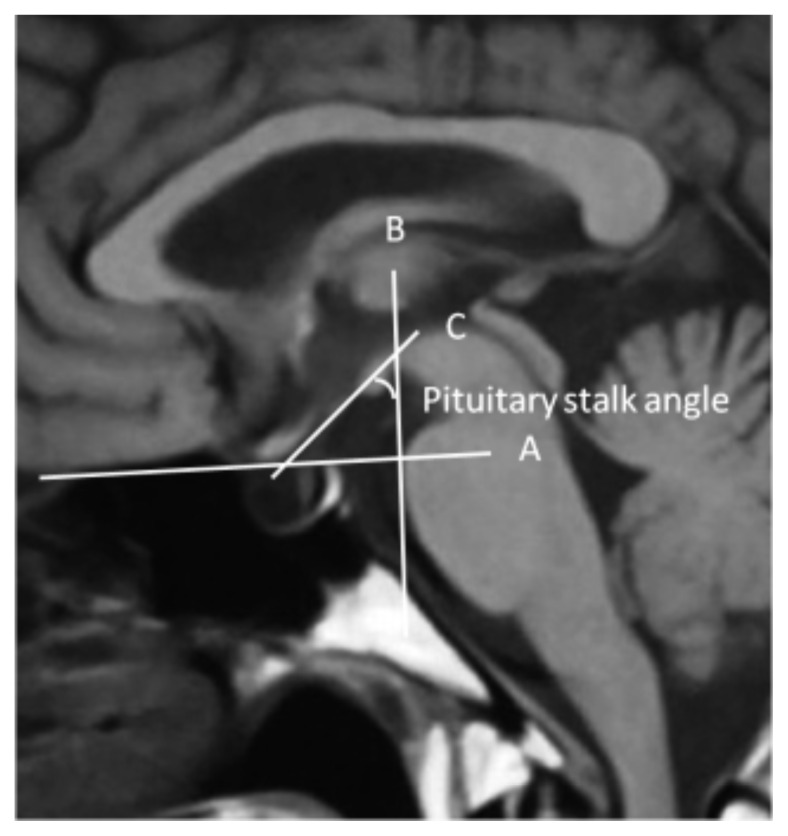
Methods: This prospective, descriptive study was conducted in the Department of Neurosurgery, General Hospital Kuala Lumpur from Jan 1, 2011 to Jan 1, 2013. Forty patients fulfilling the inclusion criteria were enrolled. All patients underwent endoscopic transphenoidal resection of non-functioning pituitary macroadenoma. Pituitary stalk angle, tumour volume and extent of tumour growth were measured from Magnetic Resonance Imaging (MRI) pre- and post-operatively. These variables were compared to serum prolactin levels measured pre and post operatively. SPSS 21 was used to perform statistical analyses.
Results: In 40 patients, the mean tumour volumes were 10.58 cm(3) (SD 7.81) pre-operatively and 3.1 cm(3) (SD 3.45) post-operatively. There was a 70% reduction in tumour volume post-operatively (P < 0.01). The mean serum prolactin was 457 mIU/L (SD 66.93) pre-operatively and 297 mIU/L (SD 6.73) post-operatively. There was a 65% reduction in prolactin serum levels after surgery (P < 0.01). The mean pituitary stalk angles were 93.45 ± 3.89 degrees pre-operatively and 51.45 ± 1.46 degrees post-operatively (P = 0.01). The mean pituitary stalk angle in the control group was 50.4 ± 8.80 degrees. Hence, there was a 98% reduction in pituitary stalk angle after surgery (P < 0.01). This study showed a linear correlation between the pre-operative and post-operative tumour volumes and serum prolactin levels (P = 0.01 pre-and post-operative) and between serum prolactin levels and pituitary stalk angle (P = 0.20 pre-operative; P = 0.01 post-operative).
Conclusion: Tumour volume and pituitary stalk angle displacement have positive predictive values for disconnection hyperprolactinemia in non-functioning pituitary macroadenoma. However, a larger sample size and further objective studies are needed to confirm these findings.
Keywords: disconnection hyperprolactinemia; pituitary macroadenoma; stalk effect.
Figures

Similar articles
-
The pituitary stalk effect: is it a passing phenomenon?J Neurooncol. 2014 May;117(3):477-84. doi: 10.1007/s11060-014-1386-5. Epub 2014 Feb 19. J Neurooncol. 2014. PMID: 24549751
-
Time Course of Resolution of Hyperprolactinemia After Transsphenoidal Surgery Among Patients Presenting with Pituitary Stalk Compression.World Neurosurg. 2017 Jan;97:2-7. doi: 10.1016/j.wneu.2016.09.066. Epub 2016 Sep 23. World Neurosurg. 2017. PMID: 27671881
-
Nonfunctioning pituitary macroadenoma presenting with mild hyperprolactinemia and amenorrhea.Fertil Steril. 1999 Oct;72(4):663-5. doi: 10.1016/s0015-0282(99)00331-3. Fertil Steril. 1999. PMID: 10521106
-
Pituitary stalk changes on magnetic resonance imaging following pituitary adenoma resection using a transsphenoidal approach.Front Neurol. 2023 Jan 27;14:1049577. doi: 10.3389/fneur.2023.1049577. eCollection 2023. Front Neurol. 2023. PMID: 36779061 Free PMC article.
-
Hyperprolactinemia: pathophysiology and management.Treat Endocrinol. 2003;2(1):23-32. doi: 10.2165/00024677-200302010-00003. Treat Endocrinol. 2003. PMID: 15871552 Review.
Cited by
-
Mechanisms of Central Hypogonadism.Int J Mol Sci. 2021 Jul 30;22(15):8217. doi: 10.3390/ijms22158217. Int J Mol Sci. 2021. PMID: 34360982 Free PMC article. Review.
-
Retrospective analysis of 52 patients with prolactinomas following endoscopic endonasal transsphenoidal surgery.Medicine (Baltimore). 2018 Nov;97(45):e13198. doi: 10.1097/MD.0000000000013198. Medicine (Baltimore). 2018. PMID: 30407358 Free PMC article.
References
-
- Arafah BM, Kailani SH, Nekl KE, Gold RS, Selman WR. Immediate recovery of pituitary function following transsphenoidal resection of pituitary macroadenomas. J Clin Endocrinol Metab. 1994;79(2):348–354. doi: http://dx.doi.org/10.1210/jcem.79.2.8045946. - DOI - PubMed
-
- Arafah BM, Nekl KE, Gold RS, Selman WR. Dynamics of prolactin secretion in patients with hypopituitarism and pituitary macroadenomas. J Clin Endocrinol Metab. 1995;80(12):3507–3512. doi: http://dx.doi.org/10.1210/jcem.80.12.8530591. - DOI - PubMed
-
- Albuquerque FC, Hinton DR, Weiss MH. Excessively high prolactin level in a patient with a nonprolactin-secreting adenoma. J Neurosurg. 1998;89(6):1043–1046. - PubMed
-
- Lees PD, Pickard JD. Hyperprolactinemia, intra-sellar pituitary tissue pressure, and the pituitary stalk compression syndrome. J Neurosurg. 1987;67(2):192–196. - PubMed
LinkOut - more resources
Full Text Sources