

Severe TSH Elevation and Pituitary Enlargement After Changing Thyroid Replacement to Compounded T4/T3 Therapy
- PMID: 27540557
- PMCID: PMC4973410
- DOI: 10.1177/2324709616661834
Severe TSH Elevation and Pituitary Enlargement After Changing Thyroid Replacement to Compounded T4/T3 Therapy
Abstract
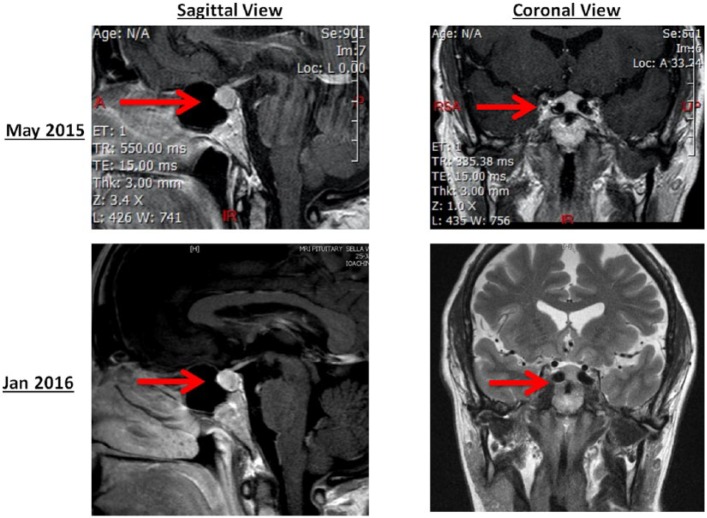
We present the first case of iatrogenic hypothyroidism as a result of compounded thyroid hormone (T4/T3) therapy. The thyroid replacement was changed from 175 µg levothyroxine (LT4) to 57/13.5 µg compounded T4/T3 daily in order to improve the T3 level, despite normal thyroid-stimulating hormone (TSH). This resulted in clinical manifestations of hypothyroidism and high TSH level (150 µIU/mL). Six months later, the patient was referred to our clinic for abnormal pituitary magnetic resonance imaging. On reinitiating a physiologic dose of LT4, clinical and biochemical abnormalities resolved and the pituitary gland size decreased. Our case emphasizes the importance of using TSH level to gauge dose adjustments in primary hypothyroidism. Also, it underscores the current American Thyroid Association recommendation against routine use of compounded thyroid hormone therapy.
Keywords: compounded T4/T3; hypothyroidism; levothyroxine; pituitary enlargement; pituitary hyperplasia.
Conflict of interest statement
Figures
Similar articles
-
MRI-demonstrable regression of a pituitary mass in a case of primary hypothyroidism after a week of acute thyroid hormone therapy.J Clin Endocrinol Metab. 1997 Mar;82(3):808-11. doi: 10.1210/jcem.82.3.3796. J Clin Endocrinol Metab. 1997. PMID: 9062487
-
Difference in pituitary-thyroid feedback regulation in hypothyroid patients, depending on the severity of hypothyroidism.J Clin Endocrinol Metab. 1978 Sep;47(3):560-5. doi: 10.1210/jcem-47-3-560. J Clin Endocrinol Metab. 1978. PMID: 263732
-
Diagnosis and treatment of hypothyroidism in TSH deficiency compared to primary thyroid disease: pituitary patients are at risk of under-replacement with levothyroxine.Clin Endocrinol (Oxf). 2011 Jun;74(6):744-9. doi: 10.1111/j.1365-2265.2011.03984.x. Clin Endocrinol (Oxf). 2011. PMID: 21521256
-
The Swinging Pendulum in Treatment for Hypothyroidism: From (and Toward?) Combination Therapy.Front Endocrinol (Lausanne). 2019 Jul 9;10:446. doi: 10.3389/fendo.2019.00446. eCollection 2019. Front Endocrinol (Lausanne). 2019. PMID: 31354624 Free PMC article. Review.
-
[Hypothyroidism--clinical findings, diagnosis, therapy. Thyroid tests should be performed on broad indications].Lakartidningen. 1998 Sep 16;95(38):4091-6. Lakartidningen. 1998. PMID: 9772803 Review. Swedish.
Cited by
-
Pituitary Hyperplasia in Severe Primary Hypothyroidism: A Case Report and Review of the Literature.Case Rep Endocrinol. 2019 Jun 25;2019:2012546. doi: 10.1155/2019/2012546. eCollection 2019. Case Rep Endocrinol. 2019. PMID: 31341683 Free PMC article.
-
Pituitary Hyperplasia Due to Longstanding Primary Hypothyroidism: A Case Report and Comprehensive Review of the Literature.Biomedicines. 2024 Jun 19;12(6):1368. doi: 10.3390/biomedicines12061368. Biomedicines. 2024. PMID: 38927575 Free PMC article.
-
Letter to the Editor: Clinically Significant Hyperthyroidism and Hypothyroidism Following Exposure to Compounded Thyroid Products.Thyroid. 2021 Jan;31(1):143-146. doi: 10.1089/thy.2020.0544. Epub 2020 Sep 18. Thyroid. 2021. PMID: 32838690 Free PMC article. No abstract available.
-
Management of hypothyroidism with combination thyroxine (T4) and triiodothyronine (T3) hormone replacement in clinical practice: a review of suggested guidance.Thyroid Res. 2018 Jan 17;11:1. doi: 10.1186/s13044-018-0045-x. eCollection 2018. Thyroid Res. 2018. PMID: 29375671 Free PMC article. Review.
References
-
- Pepper GM, Casanova-Romero PY. Conversion to armour thyroid from levothyroxine improved patient satisfaction in the treatment of hypothyroidism. J Endocrinol Diabetes Obes. 2014;2(3):1055.
LinkOut - more resources
Full Text Sources
Other Literature Sources
